|
Case Report
Nonocclusive mesenteric ischemia and heart failure: A case report and bowel ischemia imaging
1 Internal Medicine Resident, Serviço de Medicina Interna, Centro Hospitalar e Universitário de Coimbra, Hospital Geral, Coimbra, Portugal
2 Internal Medicine Attending, Serviço de Medicina Interna, Centro Hospitalar e Universitário de Coimbra, Hospital Geral, Coimbra, Portugal
Address correspondence to:
Ana Cristina Pereira Martins
Rua Dr António José de Almeida, Nº 329, 8º andar, apt 4, 3000-045 Coimbra,
Portugal
Message to Corresponding Author
Article ID: 100066Z06AM2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Martins ACP, Ribeiro P. Nonocclusive mesenteric ischemia and heart failure: A case report and bowel ischemia imaging. Case Rep Int 2019;8:100066Z06AM2019.ABSTRACT
Introduction: Mesenteric ischemia is caused by blood flow that is insufficient to meet the metabolic demands of visceral organs. When severe and prolonged, it leads to intestinal necrosis, and eventually patient death. Nonocclusive mesenteric ischemia comprises all forms of mesenteric ischemia with patent mesenteric vessels. Many etiologies have been associated: shock, heart failure, use of vasopressors. A high index of suspicion is required, since initial symptoms are vague, being the most common a gradually worsening abdominal pain. Abdominal computed tomography (CT) angiography makes the diagnosis, showing signs of bowel ischemia in the face of patent mesenteric vessels. Treatment is based on correction of the underlying cause, supportive therapy, vasodilation, and surgery. Even when treated, nonocclusive mesenteric ischemia has a mortality rate of 73–86%, being the deadliest type of acute mesenteric ischemia (AMI).
Case Report: The authors present a challenging case of AMI, in an elderly woman, with multiple cardiovascular risk factors and comorbidities. In the light of the clinical picture and the absence of mesenteric vessels obstruction, in the abdominal CT, a nonocclusive cause due to heart failure was diagnosed. However, the patient already presented with imagiological signs of advanced bowel ischemia (aeroportia and pneumatosis intestinalis), associated with a poor prognosis and a high mortality that confirmed itself.
Conclusion: This case highlights the challenges in the diagnosis of AMI, particularly when a nonocclusive cause is involved, being a clear example of the high suspicion index necessary, of the difficulties of treatment and of the poor prognosis associated.
Keywords: Acute mesenteric ischemia, Aeroportia, Heart failure, Nonocclusive mesenteric ischemia, Pneumatosis intestinalis
INTRODUCTION
Acute mesenteric ischemia (AMI) is defined as an abrupt interruption of the blood supply to the small intestine, resulting in ischemia that, when severe and prolonged, leads to intestinal necrosis, and eventually patient death [1].
Acute mesenteric ischemia may be occlusive (most commonly) or nonocclusive (NOMI) [1]. In the first scenario, vascular occlusion may be caused by an arterial embolus (40–50% of cases), an arterial thrombus (20–35%), or a venous thrombus (5–15%) [2]. In NOMI (5–15%), there is usually a low splanchnic blood flow that leads to superior mesenteric artery vasoconstriction. This can be the result of hypotension, decreased cardiac output (e.g., heart failure), or vasoconstrictors [3].
Acute mesenteric ischemia remains an interdisciplinary challenge in clinical medicine, being the most critical factor influencing outcomes the speed of diagnosis and intervention, since the symptoms are usually nonspecific [4]. Although AMI is an uncommon cause of abdominal pain, accounting for less than one of every 1000 hospital admissions, it has an overall mortality of 60–80% [2],[3]. The diagnosis among patients with NOMI is particularly difficult and the mortality particularly high, since the condition frequently affects critically ill patients, with multiple comorbidities [3]. If a high index of suspicion is required to evoke the presumptive diagnosis of AMI that is especially true in cases of NOMI [5].
The authors describe a case of severe and advanced NOMI in an elderly patient with heart failure and the difficulties in its diagnosis and management.
CASE REPORT
An 84-year-old dependent woman, with hypertension, dyslipidemia, type 2 diabetes, morbid obesity, permanent atrial fibrillation (AF), history of myocardial infarction, chronic heart failure with reduced ejection fraction (35%), stage IIIb chronic kidney disease and constipation, is admitted to the Internal Medicine ward for treatment of a lower limb cellulitis.
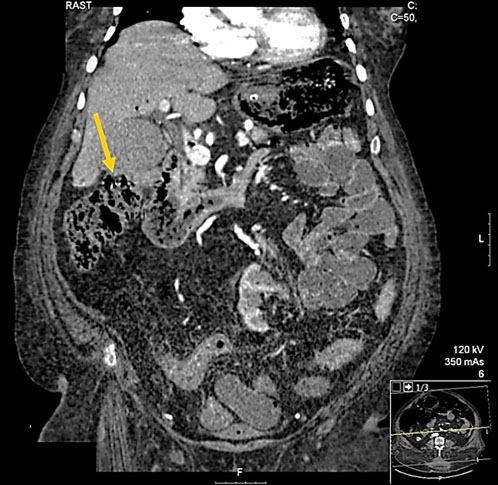
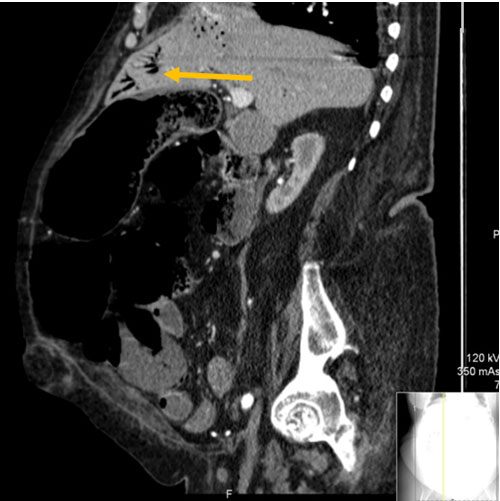
During hospitalization, the patient develops a rapid ventricular response AF with consequent decompensation of her heart failure and kidney disease. Her blood pressure (BP) is 110/60 mmHg and treatment with amiodarone and furosemide is started. Twenty-four hours later, she starts complaining of a moderate generalized abdominal pain. On exam her abdomen is tympanized and lightly tender diffusely. Her abdominal radiography shows a slightly distended colon, with no air-fluid levels or signs of perforation, that we assume to be in relation with her chronic constipation history. A few hours later, she maintains the pain, with increased intensity. Her abdomen is now more distended and markedly tender, and hematochezia is observed. Blood pressure has fallen (75/46 mmHg), and she shows clinical signs of shock. Blood gas analysis reveals a lactic acidosis (serum lactate level of 9 mmol/L). Fluids and blood transfusion are started, and an abdominal CT angiography is performed, showing a distended colon and ileum, with signs of pneumatosis intestinalis (Figure 1) and marked hepatic portal venous gas (aeroportia) (Figure 2 and Figure 3), indicating irreversible intestinal ischemia with transmural involvement. A significant atheromatous plaque of the aorta and the superior mesenteric artery is also identified, but with no identifiable thrombus or embolus.
A diagnosis of nonocclusive acute mesenteric ischemia due to heart failure is considered, and although emergency surgery is recommended, given the extension and gravity of the clinical picture, and after surgical consultation and interdisciplinary medical discussion (since the patient has no close family members), a conservative approach is taken, and the patient ultimately dies, 24 hours later.

DISCUSSION
Acute mesenteric ischemia refers to the sudden onset of intestinal hypoperfusion, which can be due to a nonocclusive reduction of arterial blood flow [6]. Nonocclusive mesenteric ischemia comprises all forms of mesenteric ischemia without occlusion of the mesenteric vessels (arteries or veins) [1],[7].
The pathogenesis of NOMI is still poorly understood, but extreme splanchnic vasoconstriction caused by a low cardiac output/hypotension in combination with diffuse atherosclerosis is probably the main pathophysiologic mechanism [3],[5]. The risk factors are diverse and include: heart failure, history of cardiac dysrhythmia or AF, diffuse atherosclerotic disease, aortic insufficiency, recent major abdominal or cardiovascular surgery, recent cardiopulmonary bypass, chronic hemodialysis, severe burns, septic shock, and the administration of vasoconstrictive medications (particularly, digoxin and epinephrine) [3],[5],[6],[7]. These explain why NOMI typically affects critically ill patients and/or elderly patients with multiple comorbidities [3],[4],[5].
In our case, the patient was an elderly woman, with various cardiovascular risk factors and chronic diseases, particularly AF and heart failure, both of which became exacerbated, during hospitalization, and ultimately led to an AMI (NOMI).
Even though NOMI accounts for 5–15% of all cases of AMI, it is a rare disease with an incidence ranging from 2/100,000 person-years in the general population to 39.8/100,000 person-years in patients aged 80 years or older [5].
Patients with AMI related to mesenteric arterial obstruction are classically described as having the typical abrupt and severe periumbilical abdominal pain out of proportion to findings on physical examination [1]. The severity and location of the abdominal pain that accompanies NOMI is usually more variable. The condition usually starts with nonspecific symptoms, consisting of mild abdominal pain that gradually progresses and may be accompanied by a bloating sensation, nausea, vomiting, diarrhea, and rectal blood loss. Abdominal pain may be absent in up to 25% of patients. Also, the clinical presentation of NOMI may be overshadowed by precipitating disorders, including hypotension, congestive heart failure, hypovolemia, and cardiac arrhythmias [6]. Physical examination often reveals a hemodynamically unstable patient with diffuse abdominal tenderness. Peritonitis is absent in the early stages of the disease, because neither the visceral nor parietal peritoneum is affected [5]. Laboratory studies are nonspecific as well. Although abnormal laboratory values, such as an elevated white cell count, elevated serum lactate, elevated hematocrit (consistent with hemoconcentration), and metabolic acidosis, may be helpful in bolstering suspicion for acute mesenteric ischemia, these do not help determine the etiology, and normal laboratory values do not exclude the diagnosis. However, any patient with acute abdominal pain, minimal findings on abdominal examination, and metabolic acidosis should be regarded as having intestinal ischemia until proven otherwise [1],[6]. Thus, a high index of suspicion is needed for diagnosis. Rapid diagnosis is essential to minimize complications (e.g., bowel necrosis, perforation) associated with intestinal ischemia [1],[2],[3].
In the case of our patient, it is clear that the NOMI process had started when she developed a mild abdominal pain and tenderness. The hypothesis of AMI was raised only when the patient was already unstable and critically ill, but given the previous clinical picture and complications, we should have considered it sooner. This clearly exemplifies the difficulty inherent to the diagnosis of AMI, and particularly of NOMI, that often delays the treatment and compromises the patient’s life.
Interestingly, in this case, despite being NOMI the main etiological hypothesis, other causes of AMI could have been considered, given the comorbidities of the patient: arterial embolic (in relation to AF and poor left ventricular function) and arterial thrombotic (in relation with the multiple cardiovascular risk factors and probable diffuse atherosclerotic disease). However, the presentation would have been different: in embolic AMI, the onset of symptoms is usually dramatic as a result of the poorly developed collateral circulation, and it is characterized by the abrupt onset of severe abdominal pain associated with diarrhea, which may become bloody; in thrombotic AMI, patients can tolerate major visceral artery obstruction because the slow progressive nature of atherosclerosis allows the development of important collaterals; bowel ischemia or infarction ensues when the last remaining visceral artery or an important collateral artery occludes. These patients usually have a history of chronic abdominal pain (abdominal angina), that ensues classically after a heavy meal, and develop an acute pain once a major/total occlusion of the mesenteric circulation occurs [1],[2] [3],[4],[8].
Multi-detector CT angiography (CTA) is the gold standard to diagnose AMI, including NOMI [1],[4]. Nonocclusive mesenteric ischemia is characterized by a diffuse spasm of the mesenteric vessels without evidence of underlying thromboembolic disease [5],[9]. Computed tomography angiography demonstrates bowel ischemia in the face of patent mesenteric vessels [1]. In the presence of advanced AMI, the CTA findings reflect irreversible ischemia (intestinal dilatation and thickness, reduction or absence of visceral enhancement, pneumatosis intestinalis, and portal venous gas) [1],[5].
In our patient, given the suspicion of AMI, a CTA was performed, revealing signs of bowel ischemia and an important aortic and superior mesenteric atheromatous plaque, but without vascular obstruction, compatible with NOMI. A diffuse pneumatosis intestinalis (gas within the bowel wall) and aeroportia (portal venous gas) were observed. These are imagiological signs traditionally associated with bowel ischemia [10]. Recently, many nonischemic causes of aeroportia and pneumatosis intestinalis were identified, usually when one of these signs presents alone [10],[11]. Despite this, the simultaneous presence of both findings is still highly predictive of bowel ischemia, frequently representing transmural involvement and a limited prognosis [12].
The goal of treatment of patients with NOMI is to restore intestinal blood flow as rapidly as possible. It is based on: treatment of the underlying cause, supportive therapy, vasodilation, and eventually surgery [1],[5],[6]. Aggressive fluid resuscitation, with crystalloid solutions, is usually required in the first hours. Placement of a nasogastric tube for gastric decompression and initiation of broad-spectrum antibiotics are also advisable [5],[6]. Although not subjected to rigorous study, antibiotics are generally recommended due to the high risk for bacterial translocation and sepsis as ischemia and/or infarction progresses [6].
Beginning of anticoagulation as a mean for improving mucosal perfusion, in the face of vasospasm, is controverse. Some clinicians anticoagulate these patients until vasoconstriction resolves and the perfusion deficit can be corrected as a means to limit the development of thrombus [6].
Vasoconstrictors are paradoxically added when the patient remains unstable after adequate fluid resuscitation, but they must be avoided, as well as digitalis, since they can exacerbate mesenteric ischemia. If inotropic agents are required, dobutamine, low-dose dopamine, or milrinone is preferred since they have less of an effect on mesenteric perfusion compared with other vasopressor agents [1],[2],[6].
Other than supportive care, the only intervention available for patients with nonocclusive mesenteric ischemia involves infusion of vasodilators to reverse splanchnic vasoconstriction [1],[5],[6]. Vasodilators can be administered either intravenously or in the superior mesenteric artery. Intravenous glucagon can be administered at a rate of 1–10 mg/kg/min, since it improves blood flow and reduces vasospasm. Intra-arterial administration of papaverine in the mesenteric blood vessels is only used when NOMI is diagnosed with mesenteric angiography. Papaverine is a phosphodiesterase inhibitor which relaxes vascular smooth muscle cells. A 60 mg bolus is followed by a constant infusion of 30–60 mg/h through the mesenteric catheter [5],[6]. Other local vasodilators include prostaglandin E1, tolazoline, and laevodosine. Vasodilator therapy is ceased when the patient’s clinical, biochemical, and radiological exams improve or after a maximum of five days [5].
If a patient presents with peritoneal signs, an exploratory laparotomy is required for resection of frankly necrotic bowel. Unfortunately, these patients are often in critical condition and the mortality remains very high (50–85%). The finding of massive gut necrosis requires careful assessment of the patients underlying comorbidities and advanced directives in order to judge whether comfort carries the best treatment [1].
Our case represents this precisely. Our patient was an elderly dependent woman, with multiple and important comorbidities, being the diagnosis of NOMI made in an advanced state of the disease, with clinical and imagiological signs of diffuse bowel ischemia with necrosis. In light of this, and after multidisciplinary discussion, the medical team assumed that supportive measures and comfort would be the best treatment approach for this particular patient.
Even though rare, NOMI has a mortality rate of 70–90% that has changed little over time, representing the poorest survival rate among the various etiologies of mesenteric ischemia, primarily because of the severity of comorbid conditions that precipitate reduced mesenteric perfusion, and delays in diagnosis [4],[6].
CONCLUSION
This clinical case intends to alert and remind clinicians of the possibility of NOMI, especially in the elderly with different comorbidities, particularly heart failure, that present with abdominal pain and clinical signs of hemodynamic instability, since the diagnostic delay and postponed treatment of this entity result in a high mortality rate.
REFERENCE
1.
Bala M, Kashuk J, Moore EE, et al. Acute mesenteric ischemia: Guidelines of the world society of emergency surgery. World J Emerg Surg 2017;12:38. [CrossRef]

2.
Clair DG, Beach JM. Mesenteric ischemia. N Engl J Med 2016;374(10):959–68. [CrossRef]
[Pubmed]
3.
Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: A clinical review. Arch Intern Med 2004;164(10):1054–62. [CrossRef]
[Pubmed]
4.
Luther B, Mamopoulos A, Lehmann C, Klar E. The ongoing challenge of acute mesenteric ischemia. Visc Med 2018;34(3):217–3. [CrossRef]
[Pubmed]
5.
Versyck G, de Gheldere C, Vanclooster P. Non-occlusive mesenteric ischemia: Two case reports and a short review of the literature. Acta Chir Belg 2018;118(6):392–7. [CrossRef]
[Pubmed]
6.
Tendler DA, Lamont JT. Nonocclusive mesenteric ischemia. UpToDate 2018. [Available at: https://www.uptodate.com/contents/nonocclusive-mesenteric-ischemia]
7.
Trompeter M, Brazda T, Remy CT, Vestring T, Reimer P. Non-occlusive mesenteric ischemia: Etiology, diagnosis, and interventional therapy. Eur Radiol 2002;12(5):1179–87. [CrossRef]
[Pubmed]
8.
Sise MJ. Mesenteric ischemia: The whole spectrum. Scand J Surg 2010;99(2):106–10. [CrossRef]
[Pubmed]
9.
Takeuchi N, Semba S, Naba K, Maeda T, Takada M. Non-occlusive mesenteric ischemia during the course of heart failure. J Clin Case Rep 2012;2:15. [CrossRef]
10.
Nelson AL, Millington TM, Sahani D, et al. Hepatic portal venous gas: The ABCs of management. Arch Surg 2009;144(6):575–81. [CrossRef]
[Pubmed]
11.
Patel NM. Hepatic portal venous gas with pneumatosis intestinalis. Gastroenterology Res 2009;2(1):51–3. [CrossRef]
[Pubmed]
12.
Liu SW, Huang TY. Portal venous gas and pneumatosis intestinalis. CMAJ 2013;185(3):E175. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ana Cristina Pereira Martins - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Pedro Ribeiro - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Ana Cristina Pereira Martins et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.