|
Case Report
A rare cause of pulmonary artery pseudoaneurysm: A case report
1 Radiology Department, Mohamed the Fifth Military Instruction Hospital, Mohamed V University, Rabat, Morocco
2 Cardiology Department, Mohamed the Fifth Military Instruction Hospital, Mohamed V University, Rabat, Morocco
Address correspondence to:
Asaad El Bakkari
Radiology Department, Mohamed the Fifth Military Instruction Hospital, Mohamed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 100073Z06AB2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
El Bakkari A, Ayouche O, Diekouadio F, el Menaoui O, Bouchaib R, Salmi N, Kettani Y. A rare cause of pulmonary artery pseudoaneurysm: A case report. Case Rep Int 2019;8:100073Z06AB2019.ABSTRACT
Introduction: An aneurysm is defined as a focal dilatation of a blood vessel involving all three layers of the vessel wall. Behçet’s disease is responsible for inflammation of the pulmonary arteries and may conduce to an aneurysm. Fifteen percent of patients with Behçet’s disease suffer from vascular involvement that includes pulmonary arteries, peripheral and central veins, peripheral and large arteries. The most common manifestation is the deep venous thrombosis (DVT) around 87%; on the other hand the involvement of the pulmonary arteries reaches 10% of the patients.
Case Report: We expose the case of a 31-year-old man, who consulted in emergency for hemoptysis that led to the performance of bronchoscopy and a bronchoalveolar lavage. To enrich the case, a thoracic computed tomography (CT) with and without enhancement and a magnetic resonance imaging (MRI) were conducted. The MRI demonstrated bilateral pseudoaneurysms of the pulmonary artery. The treatment was based on corticotherapy and hemostatic. No complications were noted in follow-up exams.
Conclusion: Pseudoaneurysm of pulmonary artery is rare, congenital heart disease and pulmonary hypertension are the leading causes. They can rupture and their management needs multidisciplinary staff.
Keywords: Aneurysm, Behçet, Computed tomography, Pulmonary artery
INTRODUCTION
Behçet’s disease is a multisystemic illness characterized by a chronic and repetitive inflammation [1]. It is responsible for variable clinical manifestations: skin and mucosa, ocular, vascular, articular, gastrointestinal, urogenital, neurologic, and pulmonary. Thoracic involvement is rare, literature data are restricted and few; however, it is considered a bad prognostic sign [2],[3].
A pseudoaneurysm is a focal dilatation that does not involve all layers of the arterial wall because of that the risk of rupture rises. Pulmonary artery pseudoaneurysms (PAPs) are unusual in front of their high morbimortality, their recognizance is fundamental. Common causes include vasculitis, infection, neoplasm, and trauma, often iatrogenic [4],[5].
On radiographs, aneurysms may appear as a lung mass or hilar enlargement. The diagnosis is usually confirmed with contrast-enhanced CT, which provides critical information for preoperative planning [6]. Magnetic resonance imaging can also show arterial wall thickening in connective tissue disease. Early recognition and treatment are important for reducing morbidity and preventing mortality.
CASE REPORT
We present the case of a 31-year-old patient, who was followed in our structure for one and half years for relapsing bipolar aphthosis. His history was characterized by a six months treatment for pulmonary tuberculosis in 2016. On admission, he presented mild hemoptysis for a period of 15 days and put under hemostatic treatment: terlipressin at 2 mg every four hours by intravenous injection in pulmonology department with drying out of his hemorrhage for four days. Moreover, there were no other neurological, articular, or digestive signs associated with it, all of which evolved in the preservation of his general state.
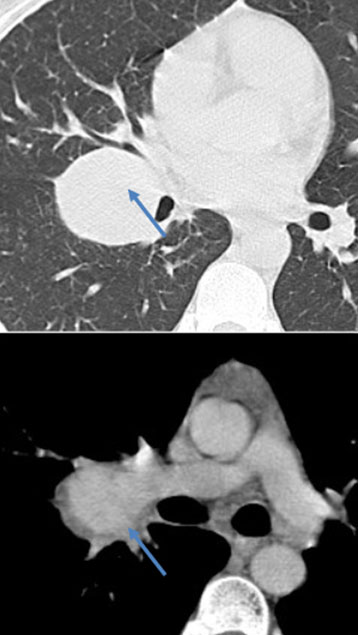
The clinical examination showed a eupneic patient in good general state with the rest of the clinical examination without abnormalities. Contrast-enhanced CT showed an aneurysm of the distal portion of the pulmonary arteries without rupture signs (Figure 1). These explorations were completed with an MRI, which had shown a pseudoaneurysm in the high signal after enhancement (Figure 2).
After a multidisciplinary consultation, the decision was for medical treatment in front of a diameter less than 6 cm and the inflammatory etiology. We opted in the first line for a bolus of methylprednisolone at 1 g, then we used per os prednisone at 60 mg per day to control the inflammatory state, besides of a hemostatic treatment like described above. The patient is currently in good shape with no further complications.

DISCUSSION
Described in 1937 by Hulusi Behçet, triad associating oral aphthosis, genital aphthosis, and uveitis. Behçet’s disease is now part of vasculitis with involvement of large or small arterial and venous vessels. Observed with preference in the countries of the Mediterranean basin and Japan, it is, in fact, ubiquitous (disease of the silk route), in Turkey, the Maghreb as high prevalence countries. Statistics show a male predominance with a sex ratio of 3:1. Young adults of 20–30 years are the most involved with some rare cases described in the pediatric populations. A genetic factor was identified and is likely given the increased frequency of HLA-B51 Ag and more recently the MIC-A gene, close to HLA class I in affected subjects, but familial cases are rare (less than 5%) [2],[7].
Pseudoaneurysms in CT are characterized by a sacciform or fusiform dilation homogenously enhanced synchronously with the pulmonary artery [8].
Behçet’s syndrome commonly results in pulmonary artery aneurysms (PAA), typically involving the right lower lobe arteries with frequent thrombosis and surrounding inflammation [9].
Although these PAAs may regress with immunosuppressive drugs, embolization is needed to prevent life-threatening hemoptysis. Other thoracic manifestations of Behçet’s syndrome include venous thrombosis, pulmonary infarction and hemorrhage, recurrent pneumonia, organizing pneumonia, eosinophilic pneumonia, and pleural effusion [10].
Pulmonary involvement, which is present in 5% of affected patients, occurs in a late stage of the disease [1]. The presence of a PAP suggests a poor prognosis, with massive hemoptysis being associated with a high mortality rate [1]. The apparent PAAs in patients with Behçet’s disease are pseudoaneurysms that arise as complications of vasculitis and transmural necrosis [11]. In most patients, the pseudoaneurysms are multiple, bilateral, saccular, and partially or completely thrombosed; the pulmonary arteries distal to the pseudoaneurysms are also thrombosed [11]. Although medical treatment with cytostatic agents and corticosteroids may cause regression of pseudoaneurysms, recurrent hemoptysis, or progression in size is common [11]. Selective transcatheter embolization is a valuable alternative to surgery [11]. The technique varies from one center to another, with some interventional radiologists using coils while others favor acrylic glue [11].
A pseudoaneurysm is a focal dilatation that does not involve all layers of the arterial wall because of that the risk of rupture rises up. When occurring it may result in massive hemoptysis that can conduce to the death, and it is worsened in the association of consolidated of the infected lung. Early recognition and minimally invasive endovascular treatment may help to reduce the associated mortality rate of PAP [12].
It is important to remember that the majority of cases of hemoptysis occur due to bronchial arterial bleeding, most often occurring in chronically infected or inflamed lung tissue, such as in patients with bronchiectasis or cystic fibrosis. This is traditionally investigated with bronchoscopy for localization of the bleeding lobe followed by catheter angiography and embolization.
The improved spatial resolution and diagnostic capabilities of arterial phase contrast-enhanced multislice CT using multiplanar reconstructions, however, are likely to favor a noninvasive diagnostic modality approach first, increasingly into the future. The CT accurate anatomical localization and the identification of the feeding artery may help to easily perform the catheterization and embolization of the feeding artery [13]. Mortality is associated to 50% of cases who benefit from conservative treatment [14].
Endovascular embolization and resection of the affected pulmonary lobe are the most commonly performed treatment options for pseudoaneurysms. The most common treatment of PAP are the embolization and pulmonary lobe resection. Postoperative complications are encountered in approximately 50% of cases and fatal outcome occurs in 20% [15].
The interventional vascular radiology techniques may obstruct the feeding artery or the sac itself by embolization or coil plays a major part in the treatment of PAP. In this case, our patient was treated successfully by conservative treatment (corticotherapy) for avoiding surgery and endovascular management [12].
Pulmonary artery aneurysms are rare, congenital heart disease and pulmonary hypertension are the leading causes in the present era. Rupture and PA dissection can occur. Although PAAs and PAPs are uncommon, knowledge of their congenital and acquired causes and radiologic manifestations is important. Assessment with contrast-enhanced CT allows accurate evaluation of PAAs and PAPs, facilitating prompt diagnosis and treatment.
A close collaboration between interventional radiologists, pulmonologists, oncologists, anesthesiologists, and critical care physicians is mandatory for optimal patient management with full therapeutic options.
CONCLUSION
Pseudoaneurysm of pulmonary artery is rare, congenital heart disease and pulmonary hypertension are the leading causes. The most dangerous complication is the rupture with deadly massive hemoptysis. Their management needs a multidisciplinary staff especially when they are related to inflammatory disease.
REFERENCE
1.
Criteria for diagnosis of Behçet’s disease. International study group for Behçet’s disease. Lancet 1990;335(8697):1078–80. [CrossRef]
[Pubmed]

2.
Mahr A, Belarbi L, Wechsler B. Population-based prevalence study of Behçet’s disease: Differences by ethnic origin and low variation by age at immigration. Arthritis Rheum 2008;58(12):3951–9. [CrossRef]
[Pubmed]
3.
Wechsler B, Huong DLT, Kieffer E. Manifestations cardiovasculaires de la maladie de Behçet. Ann Med Interne 1999;150:542–54.
4.
Fraser RS, Müller N, Colman N, Paré PD. Fraser and Paré’s Diagnosis of Diseases of the Chest. Volume 1. 4ed. Philadelphia: W.B. Saunders; 1999.
5.
Nguyen ET, Silva CI, Seely JM, Chong S, Lee KS, Müller NL. Pulmonary artery aneurysms and pseudoaneurysms in adults: Findings at CT and radiography. AJR Am J Roentgenol 2007;188(2):W126–34. [CrossRef]
[Pubmed]
6.
Remy-Jardin M, Remy J. Spiral CT angiography of the pulmonary circulation. Radiology 1999;212(3):615–36. [CrossRef]
[Pubmed]
7.
Theodoropoulos P, Ziganshin BA, Tranquilli M, Elefteriades JA. Pulmonary artery aneurysms: Four case reports and literature review. Int J Angiol 2013;22(3):143–8. [CrossRef]
[Pubmed]
8.
Tunaci M, Ozkorkmaz B, Tunaci A, Gül A, Engin G, Acuna? B. CT findings of pulmonary artery aneurysms during treatment for Behçet’s disease. AJR Am J Roentgenol 1999;172(3):729–33. [CrossRef]
[Pubmed]
9.
Erkan F, Gül A, Tasali E. Pulmonary manifestations of Behçet’s disease. Thorax 2001;56(7):572–8. [CrossRef]
[Pubmed]
10.
Hiller N, Lieberman S, Chajek-Shaul T, Bar-Ziv J, Shaham D. Thoracic manifestations of Behçet disease at CT. Radiographics 2004;24(3):801–8. [CrossRef]
[Pubmed]
11.
Cantasdemir M, Kantarci F, Mihmanli I, et al. Emergency endovascular management of pulmonary artery aneurysms in Behçet’s disease: Report of two cases and a review of the literature. Cardiovasc Intervent Radiol 2002;25(6):533–7. [CrossRef]
[Pubmed]
12.
Chellamuthu S, Bottomley JR. Treatment of a large pulmonary artery pseudoaneurysm secondary to fungal infection using Amplatzer plugs: New embolisation devices for the management of haemoptysis. Respir Med Case Rep 2012;5:78–80. [CrossRef]
[Pubmed]
13.
Kierse R, Jensen U, Helmberger H, Muth G, Rieber A. Value of multislice CT in the diagnosis of pulmonary artery pseudoaneurysm from Swan-Ganz catheter placement. J Vasc Interv Radiol 2004;15(10):1133–7. [CrossRef]
[Pubmed]
14.
Fernando HC, Stein M, Benfield JR, Link DP. Role of bronchial artery embolization in the management of hemoptysis. Arch Surg 1998;133(8):862–6. [CrossRef]
[Pubmed]
15.
McCollum WB, Mattox KL, Guinn GA, Beall AC Jr. Immediate operative treatment for massive hemoptysis. Chest 1975;67(2):152–5. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Asaad El Bakkari - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Othman Ayouche - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fabrice Diekouadio - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ouadie el Menaoui - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Redouane Bouchaib - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Najlaa Salmi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Youness Kettani - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Asaad El Bakkari et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.