 |
Case Report
Locked-in on Bora Bora—Chikungunya triggered Bickerstaff’s encephalitis mimicking brain death in French Polynesia
1 Department of Anaesthesiology and Pain Therapy, University of Bern, Bern, Switzerland
2 Rega Air Rescue, Zurich, Switzerland
3 Department of Infectiology and Hygiene, University of Zurich, Zurich, Switzerland
Address correspondence to:
Lorenz Theiler
Freiburgstrasse 4, University Hospital Bern, CH-3010 Bern,
Switzerland
Message to Corresponding Author
Article ID: 100074Z06CC2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Conrad C, Staub G, Braun D, Theiler L. Lockedin on Bora Bora—Chikungunya triggered Bickerstaff’s encephalitis mimicking brain death in French Polynesia. Case Rep Int 2020;9:100074Z06CC2020.ABSTRACT
Introduction: This is a case report about a severe neurological manifestation of a tropical disease that resulted in an overlap syndrome mimicking brain death. We are showing a Chikungunya (CHIKV)-associated encephalitis triggering an overlapping autoimmunological disease [antibody negative Bickerstaff’s brainstem encephalitis (BBE) with Miller Fisher syndrome (MFS) and Guillain–Barré syndrome (GBS)] and the resulting complications. Until recently, CHIKV was considered to cause a relatively harmless self-limiting disease with Dengue-like symptoms (DENV). This case supports the idea of likely neuroinvasiveness of CHIKV, suggesting a potential high severity of this infection. Chikungunya shows a global development and evolution from a rarely seen pathogen toward an epidemic causing disease within only a few decades.
Case Report: A 74-year-old man fell sick during his holidays in French Polynesia. He initially presented with fever and a rash, which slowly progressed to hoarseness and back pain. Within one week, the patient developed numbness of the fingertips and difficulties breathing, finally resulting in a complete irresponsive neurological state. Local physicians assumed brain death caused by a cardiac event and voted for termination of mechanical ventilatory support. However, the patient′s wife perceived responses of her husband and initiated extensive repatriation by the Swiss Air Rescue, Rega. Strikingly, the patient recovered subsequently and is wheelchair mobile today.
Conclusion: This case demonstrates how tropical airborne virus diseases become directly visible effects of global warming and globalization, as the disease recently seems to appear in Europe and America. It exemplifies how a broader knowledge of parainfectious neurologic syndromes might help to save lives by avoiding misdiagnosis or potentially fatal therapeutic decisions.
Keywords: Bickerstaff′s brainstem encephalitis, Chikungunya, Guillain–Barré syndrome, Miller Fisher syndrome
INTRODUCTION
Chikungunya is an emerging tropical virus, so far known for causing rather unspecific and self-limiting symptoms. The authors describe a unique case of a Chikungunya triggered overlap syndrome, involving GBS as an acute inflammatory flaccid peripheral paresis, MFS as the cranial nervous variant of GBS, and BBE, compromising also consciousness. It presented like brain death and therefore almost led to termination of ventilatory support, although the patient was locked-in. The courageous patient’s wife, extensive repatriation, and local intensive care treatment saved the patient’s life. Throughout the report, the authors highlight and discuss the situations that led to the diagnostic and therapeutic decisions and draw conclusions for medical staff and public health.
CASE REPORT
A 74-year-old male patient fell ill on Bora Bora in the South Pacific, presenting with fever and maculopapular exanthema, predominantly on the back. A performed test for Chikungunya and Dengue, which unfortunately was not further specified, showed negative results. The patient received paracetamol and was discharged the same day in stable clinical conditions. The patient’s relevant medical history included arterial hypertension, dyslipidaemia, former smoker (estimated 60 cumulative packyears), and occasional alcohol consumption. He underwent hemicolectomy because of adenocarcinoma in the preceding years but was considered disease free at that time. His medication consisted of a daily intake of 100 mg amino salicylic acid as primary prevention and 10/40 mg ezetimib/simvastatin.
Within the following week, the patient suffered from severe back pain, slowly progressive nausea, hoarseness, and numb feeling in the fingertips. Another 24 hours later, the patient was re-hospitalized by ambulance, apparently showing incapability of walking, impairment of consciousness, and acute respiratory insufficiency. The local medical staff also observed a ventricular tachycardia in the electrocardiogram (ECG), which led to therapy with electrical cardioversion and a single dose of amiodarone. The patient then converted back into sinus rhythm and was transported by air ambulance to Papeete on Tahiti, the capital of French Polynesia. Because of the persisting impairment of consciousness and respiratory insufficiency, the patient was intubated and connected to mechanical ventilation.
The blood test showed elevated levels of troponin, but any other laboratory values taken were not available retrospectively. The transthoracic echocardiography (TTE) showed right ventricular abnormalities with septal and apical dyskinesia and an ejection fraction (EF) of 50% (normal range 55–75%). Cranial, abdominal, and thoracic computed tomography (CT) revealed no pathological findings. On the next day, a percutaneous coronary intervention (PCI) showed an extended front wall infarction with a proximal blockage of the left anterior descending artery (LAD), which was treated with a stent. Furthermore, he received medical therapy with unselective beta-blockage (propranolol, 40 mg), dual platelet inhibition with Adenosine-diphosphate (ADP)-receptor-antagonists (clopidogrel, 75 mg) and acetylsalicylic acid [ASA, 500 mg intravenous (i.v.)], enoxaparin (0.4 mL) for prevention of thrombosis, and proton pump inhibitor (PPI, nexium, 40 mg).
An electroencephalogram (EEG) of the unconscious patient showed diffuse alpha rhythms, which were interpreted as alpha coma. The magnetic resonance imaging (MRI) of the head was without pathological findings. Cerebrospinal fluid (CSF) examination was bloody but showing negative bacteriology. The patient still had a Glasgow Coma Scale (GCS) of 3/15, even after five days without sedation. The neurological examination at this time showed no motoric or sensory reactions at all, neither spontaneous breathing nor speech or other higher mental functions. The patient showed a complete internal and external ophthalmoplegia, no pupil reaction to direct or indirect light, bifacial paresis, no motoric of the tongue, no choke-reflex, areflexia, and flaccid tetraparesis with no pyramidal tract signs. Hypoxic brain damage of unknown origin was assumed, and local doctors decided on palliative care.
However, the patient’s wife asked for repatriation, claiming to notice faint reactions like head movement when speaking loud to her husband. At this time, the Swiss Air Rescue organization Rega became involved, and the decision for costly repatriation was made. The patient finally was repatriated and admitted to the intensive care unit of the University Hospital Zurich, Switzerland. The flight took 30 hours, during which the intubated patient was always stable.
The blood test at admission in Zurich showed elevated immunoglobulin M (IgM) and immunoglobulin G (IgG) levels for CHIKV and DENV. The constellation of previous negative serology for CHIKV and DENV with subsequently positive CHIKV antibodies and DENV serology was interpreted as subacute CHIKV infection and probable post-DENV infection, or an accompanying unspecific cross-reactive DENV serology, respectively (Table 1). Zika (ZIKV) serology was always negative.
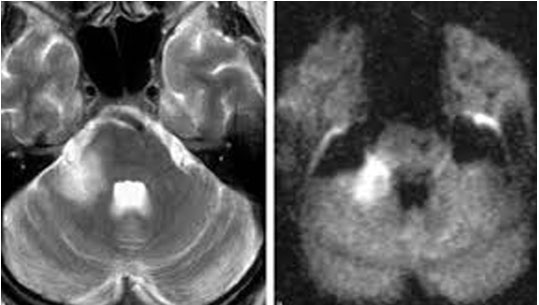
A spinal tap was repeated, which showed albuminocellular dissociation (elevated total protein without cell count abnormality) with elevated protein (2970 mg/dL; Ref.: 200–500 mg/dL), and a discrete elevation of cells (10 cells/μL, corrected because contamination with blood; Ref.: 0–4 cells/μL), interpreted as severe disturbance of the blood–brain barrier. Further CSF findings were positive oligoclonal bands together with a higher immunoglobulin A (IgA) ratio between serum and CSF than the IgG ratio, proving intrathecal IgM/IgA production, interpreted as systemic immune response (Table 1). All tested ganglioside antibodies, especially anti-GQ1b, were negative. Magnetic resonance imaging showed signal intensification involving mesencephalon, thalamus, and capsula interna with a predominance on the left side (Figure 1). Electroneurogram (ENG) and electromyogram (EMG) showed acute distal denervation with spontaneous pathological activity. In the electrophysiological examination no potentials were detectable, but the patient reacted to oration with horizontal eye movements. The EEG again was inconspicuous.
In summary, the patient suffered from a rapid progressive rhombencephalitis with complete ophthalmoplegia and fluctuating vigilance, associated with severe axonal polyneuropathy and areflexia. This led to the diagnose of overlapping antibody-negative BBE, MFS, and GBS.
The patient received intravenous immunoglobulins (IVIG, 40 g/d for five days) as well as steroids (methylprednisolone, 1 g for five days), based on the idea of autoimmunological triggered pathogenesis of the disease. The patient recovered slowly, starting with horizontal eye movements, followed by the capability of communicating by head movements. To facilitate weaning, a tracheostomy was placed, as well as a gastrostomy, and the patient was transferred to a specialized center for paraplegic patients after six weeks of intensive care, for four further months.
About five years after the incidence, the patient has mentally recovered but remaining incomplete tetraplegia, with a distally pronounced polyneuropathy and neurogenic bladder dysfunction. He is mobile in a wheelchair, capable of using his hands for writing and painting.

DISCUSSION
The case describes several challenges in the interface of retrieval medicine, tropical medicine, and intensive care between two different health care systems. In this patient, the first challenge was the initial negativity for CHIKV and DENV, which may be explained by the offset between the infection and the serology (Figure 2). The second and central challenge is the coma of the patient, which was misinterpreted as brain death and, therefore, almost led to the termination of therapy. Third, the overlap syndrome with the missing specific antibodies for the BBE impeded the final diagnosis once more. Finally, it remains elusive whether this case was a CHIKV associated encephalitis or a parainfectious phenomenon.
The underlying immunopathogenesis was most likely an acute CHIKV infection leading to the cross-reactivity based molecular mimicry of the antibodies toward the epitopes of central and peripheral neurons. This caused the brainstem encephalitis and the polyneuropathy that were altogether mimicking brain death. The positive reaction toward the treatment with steroids and immunoglobulins substantiates this thesis, as the use of steroids would not be standard of care in viral encephalitis. It remains speculative if the neurological outcome of the patient would have improved with an earlier start of therapy against the immunoreactions in analogy to treatment of sepsis or meningitis.
Published comparable cases also showed unresponsiveness to neurological stimuli (areflexia, reduced brainstem reflexes, reduced evoked potentials) and often an albumino-cellular dissociation in the CSF. These syndromes were triggered by agents, such as Dengue virus, Zika virus, or Swine flu, identified by elevated antibodies or reverse transcription polymerase chain reaction (PCR) [1],[2]. Alternatively, a bacterial genesis with Campylobacter jejuni or Haemophilus influenza as underlying pathogens was shown. Tests for ganglioside antibodies came out positive in some cases, and remained negative in others [3],[4],[5]. Neuroimaging inconsistently revealed signs of cerebral involvement. Areas of the brainstem, thalamus, and capsula interna were likely affected, presenting with higher intensity in the MRI and hypodensities in cranial CT scans. The EEG displayed alpha coma in some cases, or theta-delta slowing in one case [6],[7]. Many of the cases were reported from French Polynesia, as well as from India, and Italy [1],[6],[8],[9]. Once GBS, MFS, BBE, or overlaps were diagnosed, treatment with steroids, plasmapheresis, and intravenous immunoglobulins (IVIG) seemed standard. Patients showed slow progress under this therapy. Therapy with steroids is only indicated in case of encephalopathy or neuritis but may lead to a delayed recovery unless used in combination with IVIG [8]. Treatment with plasma exchange or IVIG is reported efficient in severe cases of, for example, CHIKV-related polyneuropathy, according to guidelines [8]. Most of the patients with a neurotropic manifestation of CHIKV and other related arboviruses show a worse outcome with persisting disabilities [4],[7],[10]. Mortality was ranging up to 48% in epidemics, even in young people with unremarkable prior medical history [10].
The central diagnostic challenge of the presented case is the local physicians’ misinterpretation of the lockedin syndrome (LIS) as brain death after the cardiac event, based on the diffuse alpha patterns in the EEG interpreted as alpha coma. Alpha coma is characterized by a complete lack of wakefulness and awareness, presenting in EEG examinations as a diffuse or widespread rhythmic activity within the alpha frequency band (8–13 Hz), typically occurring after hypoxic etiologies, cardiorespiratory arrest, or brainstem lesions with poor neurological prognosis [6],[11],[12]. Locked-in syndrome presents with tetraparesis and anarthria, as a result of disruption of corticospinal and corticobulbar pathways. The patients with incomplete LIS are commonly sensing self-awareness and remaining motoric functions, such as horizontal eye movement or blinking [11]. Locked-in syndrome is easily misdiagnosed, and the number of patients let to die without proper treatment while being fully conscious is unknown. Patients are reported to likely have a reduced motoric recovery and require specific communication strategies. Presumably, the overlap syndrome of central and peripheral nerve involvement in the presented case was simulating brain death with an absence of brainstem and peripheral reflexes, but the patient was completely locked in.
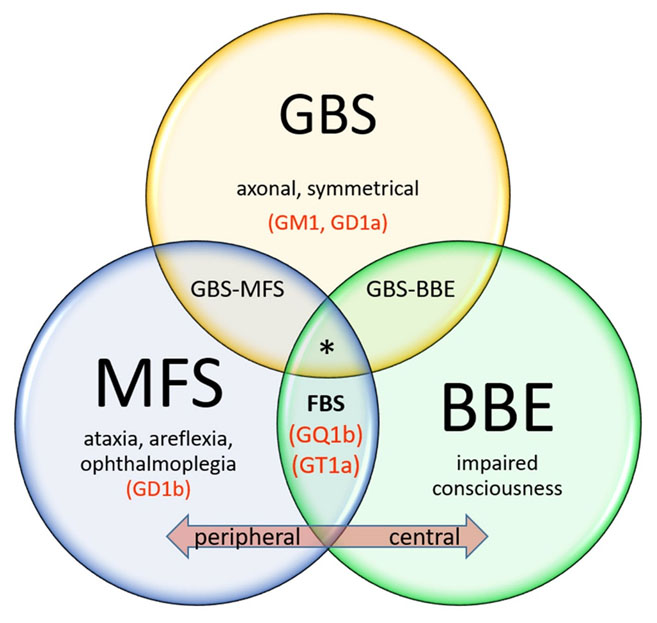
Guillain–Barré syndrome is an often infectiontriggered immune-mediated peripheral neurological demyelinating polyradiculoneuropathy, which presents typically as acute symmetrical flaccid paralysis [5]. Miller Fisher syndrome is a cranial nervous variant of GBS with a classical triad consisting of ataxia, ophthalmoplegia, and areflexia. The extreme modification is the BBE [13]. It is a rare disease with central nervous involvement showing as impaired consciousness and possibly results in total paralysis and loss of brainstem reflexes, resembling brain death [14]. The previous paragraph suggests that GBS, MFS, and BBE might be part of a continuous clinical spectrum with a high incidence of overlaps (Figure 3) [3]. Ganglioside antibodies in our presented case were negative, reflecting their low sensitivity in MFS (20%) and BBE (30%) [14].
Chikungunya is an ARthropod-BOrne (ARBO-) RNAalphavirus, transmitted by female Aedes mosquitoes that are also the reservoir for DENV, ZIKV, and Yellow fever [15]. It is presenting in seasonal outbreaks among the Pacific Ocean, with usually self-limiting unspecific symptoms of sudden onset of fever, severe arthralgia lasting from days to months, headache, lymphadenopathy, malaise, and a nonpruritic maculopapular rash, three of which the patient showed. Chikungunya virus infects over a million people per year [15]. The name Chikungunya is said to have its origin in the Tanzanian local language Makonde where it translates figuratively as “to walk bent over,” apparently due to the arthritic phenomenon.
Before 2011, the 22 Pacific Island Countries and Territories were presumed to be free of Chikungunya, as the virus originated in Africa and was introduced with increased virulence to the other continents secondary [10],[16],[17]. There are reports about a Chikungunya outbreak in French Polynesia in 2014/2015, affecting an estimated 66,000 people during the same period of this presented case [18]. They describe similar neurologic manifestations and other analogical diagnostic findings like the albumino-cellular dissociation of the CSF and negative ganglioside antibodies, suggesting the idea of the same strain of the virus. Most likely, the case described here adds to this reported epidemic. Even if we assumed a similar comparable course in only 0.1%, dozens of people would then have potentially died because of misdiagnosis.
Moreover, there is a potential for spread and outbreak due to the increasing travel and migratory exchange, climatic developments, and the dispersal of vector animals, carrying both DENV and ZIKV [16],[18]. It appeared in Italy with 86 proven cases of CHIKV in 2017 and earlier in 2007, with 205 reported cases [9]. As it seems to be a vital but unrecognized cause of coma and an underestimated emerging global threat, it is essential to keep in mind as a differential diagnosis, along with malaria and dengue fever in returning travelers.
It remains speculation if the infarction of the LAD, the heart rhythm disorders, and the fluctuations of blood pressure in the patient were causative to the CHIKVinduced overlapping postinfectious immunological triggered disease, or if the cardiac event occurred independently on top of the underlying risk factors [19].

CONCLUSION
When suspecting ARBO-virus infection, all the abovementioned should be ruled out by the healthcare providers, because of the similar presentations of the resembling diseases. In the first week after onset, serology with enzyme-linked immunosorbent assay (ELISA) is rarely helpful because of the delayed increase of the antibodies. Being aware of this potential false negativity is essential. If accessible, (RT-)PCR examinations should be performed at least in earlier stages for direct detection of the pathogenic RNA/DNA. Although there is no causal therapy for the ARBO diseases so far, the associated parainfectious triggered autoimmunological phenomena are treatable with plasmapheresis and immunoglobulins if available.
Locked-in syndrome is easily overseen, and therefore likely misdiagnosed as a coma or vegetative state. A thorough neurological examination with an accentuation on pathological respiratory patterns and brain imaging might help to differentiate between the entities.
What we could learn from this case is the importance of trusting impulses given by the relatives of our patients, in addition to measurable results. At least we should consider them instead of solely focusing on the findings provided by the medical machinery that surrounds and sometimes determines our medical field of activity.
In our globalized world, it is crucial to take CHIKV and tropical diseases in general into consideration. The CHIKV has developed from a relatively rare disease with few complications to an epidemic disease with severe progression within the last few decades, crossing borders and oceans without effort.
REFERENCE
1.
Watrin L, Ghawché F, Larre P, Neau JP, Mathis S, Fournier E. Guillain-Barré syndrome (42 cases) occurring during a Zika virus outbreak in French Polynesia. Medicine (Baltimore) 2016;95(14):e3257. [CrossRef]
[Pubmed]

2.
Carroll WM, Mastaglia FL. 'Locked-in coma' in postinfective polyneuropathy. Arch Neurol 1979;36(1):46–7. [CrossRef]
[Pubmed]
3.
de Bruyn A, Poesen K, Bossuyt X, et al. Clinical spectrum of the anti-GQ1b antibody syndrome: A case series of eight patients. Acta Neurol Belg 2019;119(1):29–36. [CrossRef]
[Pubmed]
4.
Lebrun G, Chadda K, Reboux AH, Martinet O, Gaüzère BA. Guillain-Barré syndrome after chikungunya infection. Emerg Infect Dis 2009;15(3):495–6. [CrossRef]
[Pubmed]
5.
Sekiguchi Y, Mori M, Misawa S, et al. How often and when Fisher syndrome is overlapped by Guillain-Barré syndrome or Bickerstaff brainstem encephalitis? Eur J Neurol 2016;23(6):1058–63. [CrossRef]
[Pubmed]
6.
Parvathy G, Suraj MM, Kabeer KA, Shaji CV. Alpha coma: A report. Neurol India 2017;65(3):640–1. [CrossRef]
[Pubmed]
7.
Tan CY, Ahmad SB, Goh KJ, Latif LA, Shahrizaila N. Overlap of Bickerstaff brainstem encephalitis/Guillain-Barré syndrome simulating brain death. Neurol India 2018;66(5):1475–80. [CrossRef]
[Pubmed]
8.
Simon F, Javelle E, Cabie A, et al. French guidelines for the management of chikungunya (acute and persistent presentations). November 2014. Med Mal Infect 2015;45(7):243–63. [CrossRef]
[Pubmed]
9.
Rezza G, Nicoletti L, Angelini R, et al. Infection with chikungunya virus in Italy: An outbreak in a temperate region. Lancet 2007;370(9602):1840–6. [CrossRef]
[Pubmed]
10.
Lemant J, Boisson V, Winer A, et al. Serious acute chikungunya virus infection requiring intensive care during the Reunion Island outbreak in 2005–2006. Crit Care Med 2008;36(9):2536–41. [CrossRef]
[Pubmed]
11.
Kaplan PW, Genoud D, Ho TW, Jallon P. Etiology, neurologic correlations, and prognosis in alpha coma. Clin Neurophysiol 1999;110(2):205–13. [CrossRef]
[Pubmed]
12.
Bragatti JA, de Moura Córdova N, Rossato R, Bianchin MM. Alpha coma and locked-in syndrome. J Clin Neurophysiol 2007;24(3):308. [CrossRef]
[Pubmed]
13.
Bickerstaff ER, Cloake PC. Mesencephalitis and rhombencephalitis. Br Med J 1951;2(4723):77–81. [CrossRef]
[Pubmed]
14.
Shahrizaila N, Yuki N. Bickerstaff brainstem encephalitis and Fisher syndrome: Anti-GQ1b antibody syndrome. J Neurosurg Psychiatry 2013;84(5):576–83. [CrossRef]
[Pubmed]
15.
Ganesan VK, Duan B, Reid SP. Chikungunya virus: Pathophysiology, mechanism, and modeling. Viruses 2017;9(12). pii: E368. [CrossRef]
[Pubmed]
16.
Nhan TX, Musso D. The burden of chikungunya in the Pacific. Clin Microbiol Infect 2015;21(6):e47–8. [CrossRef]
[Pubmed]
17.
Charrel RN, Leparc-Goffart I, Gallian P, de Lamballerie X. Globalization of chikungunya: 10 years to invade the world. Clin Microbiol Infect 2014;20(7):662–3. [CrossRef]
[Pubmed]
18.
Oehler E, Fournier E, Leparc-Goffart I, et al. Increase in cases of Guillain-Barré syndrome during a chikungunya outbreak, French Polynesia, 2014 to 2015. Euro Surveill 2015;20(48)30079. [CrossRef]
[Pubmed]
19.
Powers AM, Logue CH. Changing patterns of chikungunya virus: Re-emergence of a zoonotic arbovirus. J Gen Virol 2007;88(Pt 9):2363–77. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgement
The patient grants written consent to publish this case and the connected data. We thank him and his family for providing the data. We thank Elsevier, for granting permission to reuse Figure 2, as well as Prof. Dr. Claeys for providing permission to adapt the data of Figure 3.
Author ContributionsCarl Conrad - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gabriela Staub - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dominique Braun - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lorenz Theiler - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Carl Conrad et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



