|
Case Report
Acute respiratory distress reveals a mitral endocarditis and complete a case of pneumococcal infection of Austrian syndrome
1 Anesthesia and Intensive Care Department of Mohamed V Military Hospital of Rabat, Mohamed V University of Rabat, Souissi, Rabat, Morocco
Address correspondence to:
Salaheddine Fjouji
Anesthesia and Intensive Care Department of Mohamed V Military Hospital of Rabat,
Morocco
Message to Corresponding Author
Article ID: 100075Z06SF2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Fjouji S, Samali M, Atmani N, Doghmi N, Bakkali H, Baite A. Acute respiratory distress reveals a mitral endocarditis and complete a case of pneumococcal infection of Austrian syndrome. Case Rep Int 2020;9:100075Z06SF2020.ABSTRACT
Introduction: Infectious endocarditis caused by Streptococcus pneumonia remains rare but serious. When it is associated with meningitis and pneumonia, it is called Austrian syndrome.
Case Report: The authors describe a case of a 66-year-old female Moroccan patient who presented a congestive heart failure due to mitral valve disease after few days of hospitalization for pneumococcal meningitis associated with pneumonitis. The patient had a favorable course after combination of antibiotic therapy followed by surgical valve replacement.
Conclusion: The recognition of this syndrome allows an early diagnosis of cardiac involvement often masked and which worsens the prognosis. Mortality can be lowered by appropriate medico-surgical management.
Keywords: Austrian syndrome, Heart failure, Mitral endocarditis, Respiratory distress
INTRODUCTION
Dr. Robert Austrian described the association of an endocarditis, a meningitis, and a pneumopathy in 1957 at eight patients with a high mortality because of destruction of the aortic sigmoids [1]. Austrian syndrome is rare infectious disease caused by Streptococcus pneumonia with only a few reported cases worldwide. The severity of this syndrome is caused by raised morbidity and mortality due to heart failure and hemodynamic instability after the destruction of valves. A mortality which can reach 60% with only antibiotic treatment and which can be reduced to 32% with association of valvular replacement surgery and early medical treatment [2].
CASE REPORT
A 66-year-old female patient was hospitalized for agitation, fever, and disorder of consciousness following a few days of a respiratory signs including cough, expectoration with progressive dyspnea. She had a history of type II diabetes under insulin therapy, arterial hypertension treated by antagonists of angiotensin II receptors and diuretics, obesity and dyslipidemia treated by statins and aspirin. The physical examination found a patient with 40°C of temperature, confused, agitated, with a Glasgow score of 12, stiff neck, and symmetric photomotor reflex. No motor deficit was found. Arterial blood pressure was 150/80 mmHg and heart rate was 95 beats per minute. The pleuropulmonary evaluation found tachypnea with 30 cycles per minute, rales at auscultation predominating on the right side. Pulse oxygen saturation was 94% under oxygen flow of 4 L/min.
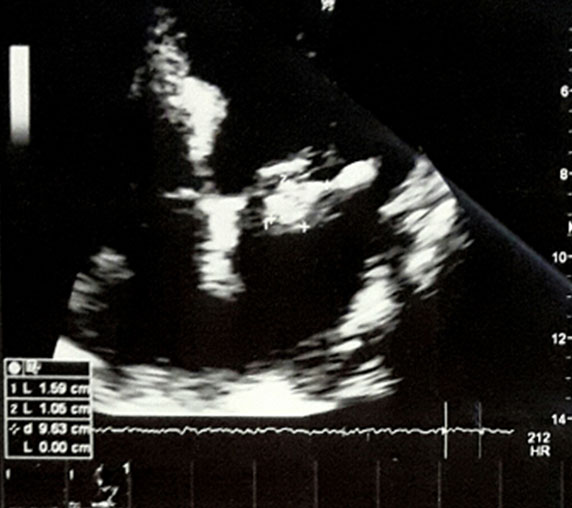
Blood sugar test was 1.9 g/L and the cranial computed tomography (CT) scan was normal. The analysis of cerebrospinal fluid showed 410 white blood cells per mm3 predominantly neutrophils, proteins at 1.45 g/L, glucose at 0.3 g/L, lactates at 14.3 mmol/L, the microscopic direct examination was negative but the pneumococcal urinary antigens were positive indicating a probably pneumococcal meningoencephalitis complicating an acute community pneumopathy. The lung disease was objectified on X-ray and thoracic CT scan that showed alveolar syndrome of the right pulmonary field without cardiomegaly (Figure 1). The biological blood test showed an acute inflammatory syndrome with leukocytes at 13,700/mm3 and a c-reactive protein (CRP) at 234 mg/L. Emergency treatment was started with ceftriaxone 8 g per day and dexamethasone 12 mg per day. After four days in intensive care, the progression was marked by an improvement in neurological status and respiratory parameters without need of oxygen support, a decrease in CRP values to 85 mg/L and white blood cells to 9200/mm3, and a radiological improvement of the lungs. Cerebrospinal fluid culture remained negative. At the eighth day, the patient had acute dyspnea with decrease of pulse oximetry at 88%. The physical examination showed a systolic murmur in the mitral focus, sibilant rales on the bilateral pulmonary fields. The chest X-ray showed a pulmonary edema with bilateral perihilar opacities. Thoracic echocardiography suspected an endocarditis by showing a hyperechoic image on the atrial aspect of the small mitral valve (Figure 2). Transesophageal echocardiography showed a small, thickened mitral valve truncated with small vegetations, a prolapse P2–P3 by cord rupture responsible of severe mitral insufficiency grade III–IV, with moderate pulmonary arterial hypertension at 37 mmHg systolic pressure (Figure 3). The left ventricle was unexpanded with good systolic function. The blood cultures remained negative. Antibiotic therapy was modified by adding vancomycin 2 g/24 h and gentamicin 160 mg/24 h associated to diuretic drugs.
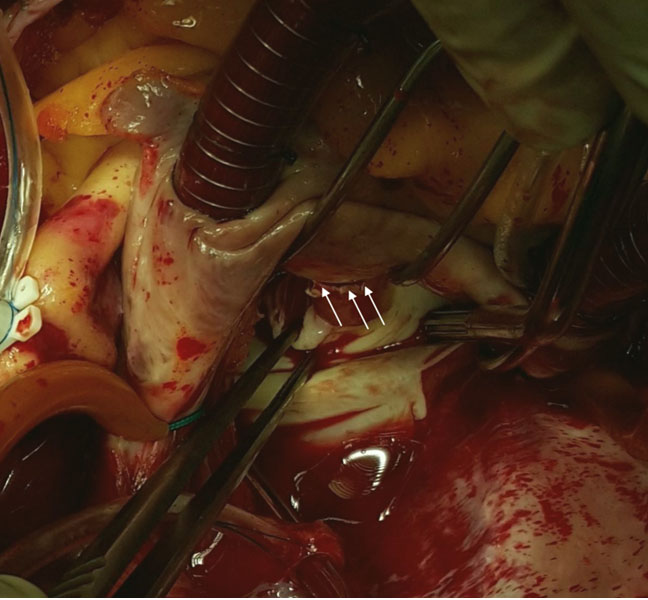
After seven days of diagnosis of endocarditis, the clinical stability and normalization of the inflammatory balance with antibiotics and diuretics allowed to consolidate the medical treatment and prepare the patient for cardiac surgery. The patient was operated as a delayed emergency. After sternotomy and establishment of conventional extracorporeal circulation, the exploration found P2–P3 prolapse by ruptured cords and a free edge of the small mitral valve filled with tiny vegetations (Figure 4). Conservative treatment was not possible and a mitral valvular replacement by mechanical prosthesis was performed. The operative follow-up and the stay in resuscitation were without serious complication. The culture of the valve allowed the isolation of pneumococcus with intermediate resistance to the penicillin. Antibiotic therapy was maintained for six weeks for vancomycin, ceftriaxone for three weeks, and gentamycin for one week.


DISCUSSION
Streptococcus pneumoniae is a rare cause of infectious endocarditis between 0.9% and 8% [3], whereas it is the most common cause of meningitis in adults [4]. It is also noted that the endocardium is a very rare localization of S. pneumoniae infection with a frequency of 0.6% [5]. The Austrian syndrome is much rarer based on cases reported in the literature estimated at 1.2% of infectious endocarditis [6]. Aronin et al. found a triad frequency of 42% of pneumococcal infectious endocarditis with mortality exceeding 50% [2]. In Morocco, only one case was reported in 2011 by Atmani et al. [7]. Austrian syndrome was widely reported in patients with a history of chronic alcoholism or intravenous drug use. Other risk factors, such as HIV immunodeficiency, cirrhosis, diabetes, splenectomy, and glucocorticoid therapy, have been described [6],[8]. Our patient was followed for type II diabetes under insulin therapy. In some cases, no obvious risk factor has been found [9]. The cardiac complication in the Austrian syndrome is the most serious and determined the prognosis outside the respiratory and meningeal attack. This is a destruction of the valves with a predilection on the aortic valves of about 75% responsible for congestive heart failure [10]. The cardiac clinical picture is generally acute and follows meningeal and respiratory involvement. Sometimes it can appear late after a meningitis [11]. Mitral valve involvement is less common than that of aortic sigmoids. This is the case of our patient who had stage II mitral insufficiency responsible for acute pulmonary edema responding favorably to initial medical treatment. Other local cardiac complications, such as abscesses, fistulas, or suppurative pericarditis, are described [10],[12]. The prognosis also depends on the early diagnosis. Some factors can participate to delayed diagnosis of endocarditis and worsen prognosis. Peripheral signs of infectious endocarditis are usually absent and major signs are predominantly with neuromeningeal and respiratory involvement. It is required to repeat clinical examinations to detect a new heart murmur or pulmonary rales if patient presents meningitis associated to pneumopathy. Echocardiography plays an important role in diagnosis. Transesophageal echography is superior to transthoracic for detecting vegetations, abscesses, and perforations [13]. It also makes it possible to evaluate the valve leak and to indicate the surgical intervention. Medical treatment with antibiotics should be initiated early. In view of the resistance to penicillin, a third-generation cephalosporin is most often used in combination with vancomycin depending on the resistance of the pneumococcus to cephalosporins [2]. High dose corticosteroid therapy has shown an improvement in the course of bacterial meningitis [14]. Despite appropriate antibiotic therapy, mortality in the absence of surgical treatment can reach 60%. It is reduced to 32% in case of surgery [2]. The majority of authors recommend surgery once a diagnosis of endocarditis is made with congestive heart failure [15]. This treatment is usually based on a valvular replacement. This surgery is often urgent, but in some cases, such as the case of our patient, it is necessary to measure the balance of an emergency surgical indication and the benefit of preoperative medical optimization [9].
CONCLUSION
The early recognition of Austrian syndrome is crucial for optimizing treatment that combines medical means and surgical management that can improve the prognosis. The authors advise a search for infectious endocarditis in cases of meningitis associated with or close to an episode of pneumonia and appeared in people with risk of pneumococcal infection.
REFERENCE
1.
Austrian R. Pneumococcal endocarditis, meningitis, and rupture of the aortic valve. AMA Arch Intern Med 1957;99(4):539–44.
[Pubmed]

2.
Aronin SI, Mukherjee SK, West JC, Cooney EL. Review of pneumococcal endocarditis in adults in the penicillin era. Clin Infect Dis 1998;26(1):165–71. [CrossRef]
[Pubmed]
3.
Lindberg J, Schønheyder HC, Møller JK, Prag J. Incidence of pneumococcal endocarditis: A regional health register-based study in Denmark 1981–1996. Scand J Infect Dis 2005;37(6–7):417–21. [CrossRef]
[Pubmed]
4.
Auburtin M, Porcher R, Bruneel F, et al. Pneumococcal meningitis in the intensive care unit: Prognostic factors of clinical outcome in a series of 80 cases. Am J Respir Crit Care Med 2002;165:713–7. [CrossRef]
[Pubmed]
5.
Kan B, Ries J, Normark BH, et al. Endocarditis and pericarditis complicating pneumococcal bacteraemia, with special reference to the adhesive abilities of pneumococci: Results from a prospective study. Clin Microbiol Infect 2006;12(4):338–44. [CrossRef]
[Pubmed]
6.
Gonzalez-Juanatey C, Testa A, Mayo J, Gonzalez-Gay MA. Austrian syndrome: Report of two new cases and literature review. Int J Cardiol 2006;108(2):273–5. [CrossRef]
[Pubmed]
7.
Atmani N, Ait Houssa M, Drissi M, et al. Syndrome d’Austrian: À propos d’un cas et revue de la littérature. Chirurgie Thoracique Cardio-vasculaire 2011;15(2):123–5.
8.
Taylor SN, Sanders CV. Unusual manifestations of invasive pneumococcal infection. Am J Med 1999;107(1A):12S–27. [CrossRef]
[Pubmed]
9.
Atkinson K, Augustine DX, Easaw J. Austrian syndrome: A case report and review of the literature. BMJ Case Rep 2009;2009. pii: bcr03.2009.1724. [CrossRef]
[Pubmed]
10.
Vindas-Cordero JP, Sands M, Sanchez W. Austrian’s triad complicated by suppurative pericarditis and cardiac tamponade: A case report and review of the literature. Int J Infect Dis 2009;13(1):e23–5. [CrossRef]
[Pubmed]
11.
Kim YM, Kim SA, Kim MG, et al. Austrian syndrome with a delayed onset of heart failure. J Cardiovasc Ultrasound 2011;19(1):35–7. [CrossRef]
[Pubmed]
12.
Luzzati R, Pinamonti B, Giacomazzi D, Sinagra G, Zingone B. Aortic-right atrium fistula complicating Austrian Syndrome: A case report and literature review. Infez Med 2007;15(2):124–8.
[Pubmed]
13.
Poulsen JB, Moser C, Espersen K, Moller K. Austrian syndrome. BMJ Case Rep 2011;2011. pii: bcr0920103368. [CrossRef]
[Pubmed]
14.
de Gans J, van de Beek D; European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. N Engl J Med 2002;347(20):1549–56. [CrossRef]
[Pubmed]
15.
Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): Developed in collaboration with the Society of Cardiovascular Anesthesiologists: Endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 2006;114(5):e84–231. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Salaheddine Fjouji - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mehdi Samali - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nourredine Atmani - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nawfal Doghmi - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hicham Bakkali - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Abdelouahad Baite - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Salaheddine Fjouji et al.. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.