|
Case Report
Left lower abdominal pain in a premenarchal girl: A case of ovarian torsion
1 General Surgical Registrar, Department of Surgery, Northern Hospital, Melbourne, Victoria, Australia
2 Consultant Paediatric Surgeon, Department of Surgery, Northern Hospital, Melbourne, Victoria, Australia
Address correspondence to:
Chao Cheng
185 Cooper Street, Epping, Melbourne, Victoria 3076,
Australia
Message to Corresponding Author
Article ID: 100076Z06CC2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cheng C, Condron S. Left lower abdominal pain in a premenarchal girl: A case of ovarian torsion. Case Rep Int 2020;9:100076Z06CC2020.ABSTRACT
Introduction: Pediatric ovarian torsion is a rare surgical emergency. In premenarchal girls, ovarian torsion can occur with or without an ovarian cyst. Due to its nonspecific presentation, diagnosis can be very challenging.
Case Report: A healthy 9-year-old girl presented to the Emergency Department with a six day history of intermittent left sided abdominal and flank pain, associated with vomiting. She appeared well on triage, and was triaged for nonurgent review. In the Emergency Department, the patient reported that she was seen by family doctor three days prior for the same symptoms and was treated for urinary tract infection with cephalexin. She denied any bowel habit changes or other systemic symptoms. She examined well, with mild tenderness over the left iliac fossa without guarding. A renal tract ultrasound was requested, and it showed a bulky left ovary with no vascular flow, suggesting ovarian torsion. The patient was subsequently taken to operating theatre and underwent laparoscopic detorsion of her left ovary. She was followed up in outpatient clinic with a pelvic ultrasound done at six weeks postoperatively which showed normal vascular flow and follicles in both ovaries.
Conclusion: In conclusion, ovarian torsion in pediatric premenarchal population is a diagnostic challenge. Abdominal ultrasound is an essential diagnostic aid, and laparoscopy with detorsion is an accepted surgical management.
Keywords: Abdominal pain, Adnexal torsion, Ovarian torsion, Pediatric, Premenarche
INTRODUCTION
Pediatric ovarian torsion is a rare but important surgical emergency, as loss of the ovary can have Long-term consequences to fertility [1], [2]. Ovarian torsion is often associated with adnexal cysts [3], and torsion of the cyst and or the ovary itself leads to presenting symptoms. Other risk factors associated with ovarian torsion include pregnancy and tubal sterilization, although both are very rare [3]. All of these risk factors are extremely rare in premenarchal patients. Overall, the clinical presentations of ovarian torsion are nonspecific, most commonly as lower abdominal pain and vomiting, making it a diagnostic challenge.
Abdominal pain is a common pediatric presentation to the emergency department. There is a long list of differentials including surgical diagnoses (e.g., appendicitis) and medical causes (e.g., viral gastroenteritis). Most children have self-limiting conditions [4], and clinical observations with analgesia are widely accepted for children presenting with nonspecific abdominal pain. It requires the treating clinician to have high index of suspicion of ovarian torsion to ensure the appropriate investigations and management are carried out in a timely manner.
Imaging, in particular ultrasound, plays an important role in diagnosing ovarian pathologies in female patients—it is especially essential if ovarian torsion is suspected. In the pediatric population, ultrasound is an essential diagnostic tool as children cannot communicate effectively with clinicians [1].
CASE REPORT
An otherwise healthy 9-year-old girl presented to Emergency Department with a six day history of intermittent left sided abdominal and flank pain, associated with vomiting. She was treated for a urinary tract infection with cephalexin three days prior by her family doctor. She reported no change in her bowel habits, and that she was systemically well.
On examination, she was afebrile and all her vitals were within normal ranges. She had mild tenderness over her left iliac fossa without guarding. She was able to ambulate within the Emergency Department without difficult; however, she reported significant pain even at rest.
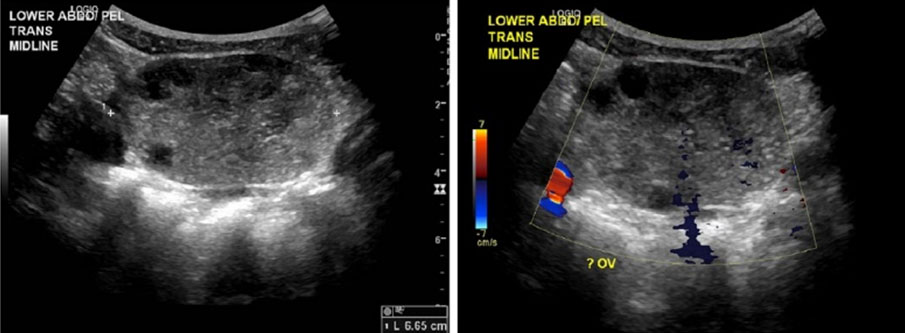
There was low suspicion of an acute surgical abdomen following assessment of this patient. An initial diagnosis of renal colic was made. The patient had a normal urinary dipstick done at the bedside, and all of her blood test results came back normal including inflammatory markers. A nonurgent renal tract ultrasound was requested after consulting the senior Emergency Physician. The ultrasound was done in a timely fashion— two hours from the time of triage, which showed a bulky left ovary without blood flows (Figure 1). The sonographer informed the emergency team as well as the acute general surgical unit promptly after scanning the patient.
Following assessment by the on call surgical registrar, the patient was taken to theatre after informed consent obtained from patient’s mother for diagnostic laparoscopy plus or minus oophorectomy. Additionally alpha fetoprotein level was negative.
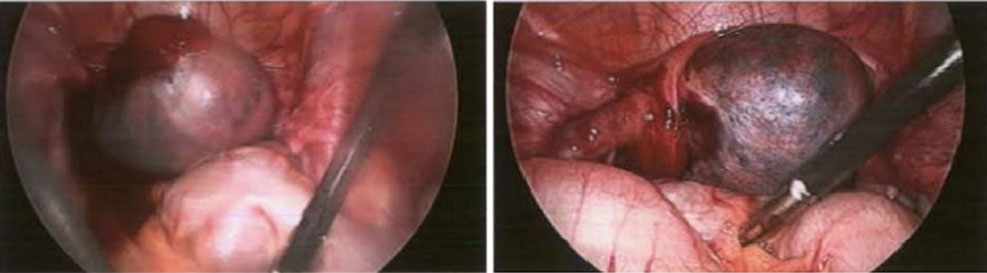
Intraoperatively, the patient was found to have a black left ovary that appeared compromised, with moderate amount of fluid in the pelvis (Figure 2). Laparoscopic detorsion was carried out and some regional color return was noted. Importantly, no malignant mass or cysts were noted on either ovaries.
The patient recovered well postoperatively, and was discharged with simple oral analgesia.
She was reviewed in outpatient clinic at two weeks postoperatively for wound check and then again six weeks with a repeat ultrasound. Ultrasound showed multiple follicles on both ovaries, and there was normal vascular flow within the left ovary.
DISCUSSION
Ovarian torsion is a rare presentation in the pediatric population [5]. A 10-year retrospective review of children (0–19 years) diagnosed with ovarian torsion at a single academic center reported incidence of 0.02% [6]; the incidence is much lower in premenarchal girls as the median age of menarche is 12 years. Although traditionally ovarian torsion is considered a postmenarchal problem, a recent retrospective cohort study [7] reported similar frequency of presentation in premenarchal and postmenarchal female patients. In particular, ovarian torsion in premenarchal girls could occur without presence of ovarian cysts.
A diagnosis of ovarian torsion is challenging due to the nonspecific symptoms and clinical signs that would mimic other abdominal conditions, such as appendicitis. A systematic review was done in 2016 to look for prediction signs of ovarian torsion. It included 14 retrospective publications, involving 663 episodes of ovarian torsion. The review reported that sudden onset of abdominal pain with nausea and/or vomiting is the most frequent presenting symptoms of ovarian torsion [8]. From the review of literature, they concluded that it is difficult to evaluate abdominal pain in pediatric population, and it was not possible to develop a diagnostic algorithm [8].
Given that patients’ clinical presentation and examination findings are nonspecific, imaging plays a key role in diagnosis [9]. In particular, ultrasound has better sensitivity picking up ovarian torsion compared to computed tomography (CT) scan (79% vs 42.2%) [8]. One study was done to analyze ultrasound determinants of adnexal torsion in children and adolescents reported that accuracy of ultrasound diagnosis was 80% with sensitivity of 90.8% and specificity of 68.7% [10]. In adult patients, ultrasound is frequently used in assessing female patients with acute lower abdominal pain. Its diagnostic value should not be ignored in pediatric population. Magnetic resonance imaging (MRI) is superior to CT due to its excellent soft tissue contrast and lack of ionizing radiation. However, the accessibility and availability of MRI is restricted in most health services.
While many pediatric patients with abdominal pain have self-resolving conditions, ovarian torsion is a time critical diagnosis that requires high index of suspicion to ensure timely treatment. Compared to testicular torsion, there is a significant delay in diagnosis and definitive treatment in ovarian torsion [6]. Boys with testicular torsion tend to have expedited management, and operative exploration is often carried out without radiologic investigations. Some advocate liberal use of diagnostic laparoscopy in girls with suspected ovarian torsion [6]. However intra-abdominal surgeries carry significant perioperative risks including anesthetic risks. With relatively high sensitivity of ultrasound in diagnosing ovarian torsion, we would recommend more liberal use of ultrasound in investigating girls presenting with abdominal pain especially those with associated vomiting.
In terms of management for ovarian torsion, oophorectomy was the standard practice; however, conservative management with ovary preservation surgery is the mainstay of current practice [11], [12], [13]. When patients were followed up after laparoscopic detorsion, 28 of 29 patients showed follicles on the affected side at eight months of follow-up [14]. An update on the management of ovarian torsion, that was done in 2015, reported that role of oophoropexy is still controversial [11]. Some reported that oophoropexy may be necessary following detorsion given the risk of recurrence [15]; however, a case series reported that recurrence may still occur after oophoropexy [16]. Current literature supports laparoscopic detorsion as a safe and effective treatment for ovarian torsion, long-term benefits especially reproductive function and outcome need to be determined for the role of oophoropexy.
CONCLUSION
Ovarian torsion in premenarchal girls is rare. Accurate diagnosis requires high index of suspicion as its clinical presentation is nonspecific. Ultrasound is a useful and important diagnostic stool. In general, detorsion without oophorectomy leads to satisfying outcome.
REFERENCE
1.
Sintim-Damoa A, Majmudar AS, Cohen HL, Parvey LS. Pediatric ovarian torsion: Spectrum of imaging findings. Radiographics 2017;37(6):1892–908. [CrossRef]
[Pubmed]

2.
Robertson JJ, Long B, Koyfman A. Myths in the evaluation and management of ovarian torsion. J Emerg Med 2017;52(4):449–56. [CrossRef]
[Pubmed]
3.
Asfour V, Varma R, Menon P. Clinical risk factors for ovarian torsion. J Obstet Gynaecol 2015;35(7):721–5.
[Pubmed]
4.
Iyer R, Nallasamy K. Child with abdominal pain. Indian J Pediatr 2018;85(1):71–6.
5.
Schwartz BI, Huppert JS, Chen C, Huang B, Reed JL. Creation of a composite score to predict adnexal torsion in children and adolescents. J Pediatr Adolesc Gynecol 2018;31(2):132–7. [CrossRef]
[Pubmed]
6.
Piper HG, Oltmann SC, Xu L, Adusumilli S, Fischer AC. Ovarian torsion: Diagnosis of inclusion mandates earlier intervention. J Pediatr Surg 2012;47(11):2071–6. [CrossRef]
[Pubmed]
7.
Schuh AM, Klein EJ, Allred RJ, Christensen A, Brown JC. Pediatric adnexal torsion: Not just a postmenarchal problem. J Emerg Med 2017;52(2):169–75. [CrossRef]
[Pubmed]
8.
Rey-Bellet Gasser C, Gehri M, Joseph JM, Pauchard JY. Is it ovarian torsion? A systematic literature review and evaluation of prediction signs. Pediatr Emerg Care 2016;32(4):256–61. [CrossRef]
[Pubmed]
9.
Naffaa L, Deshmukh T, Tumu S, Johnson C, Boyd KP, Meyers AB. Imaging of acute pelvic pain in girls: Ovarian torsion and beyond. Curr Probl Diagn Radiol 2017;46(4):317–29. [CrossRef]
[Pubmed]
10.
Jourjon R, Morel B, Irtan S, et al. Analysis of clinical and ultrasound determinants of adnexal torsion in children and adolescents. J Pediatr Adolesc Gynecol 2017;30(5):582–90. [CrossRef]
[Pubmed]
11.
Nur Azurah AG, Zainol ZW, Zainuddin AA, Lim PS, Sulaiman AS, Ng BK. Update on the management of ovarian torsion in children and adolescents. World J Pediatr 2015;11(1):35–40. [CrossRef]
[Pubmed]
12.
Laganà AS, Sofo V, Salmeri FM, et al. Oxidative stress during ovarian torsion in pediatric and adolescent patients: Changing the perspective of the disease. Int J Fertil Steril 2016;9(4):416–23. [CrossRef]
[Pubmed]
13.
Spinelli C, Piscioneri J, Strambi S. Adnexal torsion in adolescents: Update and review of the literature. Curr Opin Obstet Gynecol 2015;27(5):320–5. [CrossRef]
[Pubmed]
14.
Santos XM, Cass DL, Dietrich JE. Outcome following detorsion of torsed adnexa in children. J Pediatr Adolesc Gynecol 2015;28(3):136–8. [CrossRef]
[Pubmed]
15.
Bertozzi M, Magrini E, Bellucci C, Riccioni S, Appignani A. Recurrent ipsilateral ovarian torsion: Case report and literature review. J Pediatr Adolesc Gynecol 2015;28(6):e197–201. [CrossRef]
[Pubmed]
16.
Comeau IM, Hubner N, Kives SL, Allen LM. Rates and technique for oophoropexy in pediatric ovarian torsion: A single-institution case series. J Pediatr Adolesc Gynecol 2017;30(3):418–21. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Chao Cheng - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sarah Condron - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Chao Cheng et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.