|
Case Report
Bilateral carotid ischemia by probable strangulation in an infant: About a case and review of the literature
1 Neurosurgery Department, Fann’s University Hospital Center, Dakar, Senegal
2 Radiology Department, Fann’s University Hospital Center, Dakar, Senegal
Address correspondence to:
Yakhya Cisse
Fann’s University Hospital Center, Cheikh Anta DIOP Street, PB: 5035, Dakar,
Senegal
Message to Corresponding Author
Article ID: 100089Z06CY2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cisse Y, Mbaye T, Mohameth F, Essosolim B, Fatoumata BL, Boubakar BS. Bilateral carotid ischemia by probable strangulation in an infant: About a case and review of the literature. Case Rep Int 2020;9:100089Z06CY2020.ABSTRACT
Introduction: Strangling an infant is one of the most common methods of murder. Although rare, it remains a serious condition because of its complications.
Case Report: We report a 3-month-old infant, probably strangled, who was admitted to Fann′s emergency service with altered consciousness 10 hours prior to admission. Computed tomography (CT) scan showed a range of hypodensity in the carotid territories. The victim died later of secondary complications.
Conclusion: Infant strangulation injuries are often fatal. Management must also include forensic aspects.
Keywords: Carotid ischemia, Complications, Infant, Strangulation
INTRODUCTION
In the West, strangulation has long been the most outdated and most frequently used method of murder [1],[2]. Strangulation in children, although rare, remains a serious and potentially life-threatening condition with associated complications [3]. We report the case of a 3-month-old infant that we managed.
CASE REPORT
This is a 3-month-old male infant, the eldest son of two middle school teachers, with no particular pathological history. He was brought by his parents to the emergency service of the Fann’s University Hospital Center for consciousness disorders that had been evolving since 10 hours before his admission.
The circumstances surrounding the occurrence remain unclear. The child was in the care of a nanny. In the evening, the parents had found the inert child next to the maid. The maid could not give any explanation for the child’s condition.
The intake examination revealed tachycardia at 145 beats/min, blood pressure at 80/50 mmHg, respiration rate at 30 cycles/min, weight of 5.7 kg, and height of 60 cm.
The neurological examination had revealed: disturbances of consciousness with a pediatric Glasgow coma scale at 9/15, damage to the 3rd cranial pair on the right with ptosis and mydriasis, mobilization of the 4 limbs on stimulation, muscle tone was normal, tendon reflexes were lively and there was no cervical spinal syndrome.
Examination of the cephalic part revealed a slight puffiness of the face associated with a circumferential bruise area (Figure 1).
In addition, there were skin’s signs of mechanical compression in the lower cervical region with subcutaneous emphysema. The rest of the examination was unremarkable hemostasis assessment.
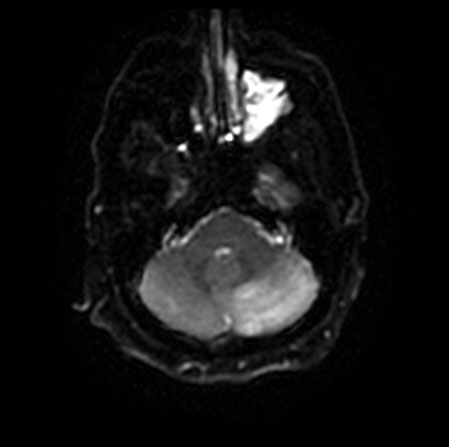
The cerebral CT scan carried out had made it possible to objectify a range of bilateral subcortical hypodensity under the fronto-temporo-parietal cortex involving the lenticular and caudate nuclei, sparing the thalamus, the occipital lobe, and the posterior fossa (Figure 2). The diagnosis of probable bilateral carotid ischemia by strangulation was made.
The child was admitted to intensive care for further treatment. Four hours after admission, the infant presented a worsening of his clinical condition with a pediatric Glasgow coma scale at 6/15, bradycardia at 50 beats/min, respiratory distress with 70% O2 saturation and polypnea at 80 cycles/min, hypothermia at 35.6 °C, requiring intubation and sedation.
Neurosurgical abstention was indicated due to the bilateral and diffuse nature of the lesions and the child died 24 hours later after admission to intensive care.


DISCUSSION
Illegal killings of infants are an emotional burden on the victim’s family and are widely reported in the media. The incidence of strangulation-related infant deaths in Africa is not well known. However, it is 55.9% in the Mathews [4] series in South Africa. Data were also found in other countries outside Africa: Verma [5] in India had an incidence of 22.4%, Sabo [6] in Peoria had 7.4%, Nixon [7] in England and Wales was 8.08% (11 cases out of a total of 136). In America Shapiro-Mendoza et al. reported a death rate linked to accidents by strangulation and suffocation varying between 2.8 and 12.5 deaths per 100,000 live births [8]. Strangulation is more common in the pediatric population [6] and is often linked to homicides [5],[7],[8]. Boys are more victims of death by strangulation [5],[8],[9],[10]. In our case it would most likely be manual strangulation. However, in the literature review, strangulation by ligature is 3 times higher than manual strangulation [4]. In our case the infant had no associated cervical bone lesion, which can be explained by the elasticity of these bones [11]. The site of injury was often cephalic and was in 20% of lacerations, abrasions, and bruises [6]. The superficial location of the carotid arteries makes it easily susceptible to compression during strangulation. On the other hand, the vertebral arteries are relatively protected by their location in the foramina [2]. This explains the ischemic territory found in our case. In some studies, lesions causing carotid obstruction in infants are rare [6],[12],[13]. Intracranial hypertension is rarely present on admission; however, late onset can occur within 24 hours leading to cerebral death [14]. The occurrence of secondary systemic stroke after strangulation is the major element to be tracked and treated to avoid progression to death [15]. At admission, the following are defined as indications of poor prognosis: prolonged coma, presence of seizures, diabetes insipidus, and hyperglycemia [4]. In our case, only consciousness disorders were found as part of the poor prognosis. Its management will have to include forensic aspects including medical reports and a judicial inquiry. In our case, an investigation is conducted with a view to charging the maid. Once the child is found, the neck examination should be performed at the scene as some artifacts may occur during transport of the child. In the Senegal Penal Code, according to the article (Law n° 76-02 of March 25, 1976), any person who illegally kills a person will be punished by death. Statements of relatives, drug addiction can provide important information on the mode and origin of death. The autopsy must be systematically carried out, since suspended cases are accepted as criminal cases [16],[17],[18],[19],[20].
CONCLUSION
Because of their serious neurological complications, strangulation injuries are often fatal in infants. The helpless condition of the infant favors homicide by manual strangulation. In the emergency department, consideration must be given not only to the management of these injuries, but also to the management of the forensic problems associated with them.
REFERENCE
1.
Cooke CT, Cadden GA, Hilton JM. Hanging deaths in children. Am J Forensic Med Pathol 1989;10(2):98–104. [CrossRef]
[Pubmed]

2.
Feldman KW, Simms RJ. Strangulation in childhood: Epidemiology and clinical course. Pediatrics 1980;65(6):1079–85.
[Pubmed]
3.
Serena K, Piva JP, Andreolio C, Carvalho PRA, da Rocha TS. Accidental strangulation in children by the automatic closing of a car window. [Article in Portuguese]. Rev Bras Ter Intensiva 2018;30(1):112–5. [CrossRef]
[Pubmed]
4.
Mathews S, Abrahams N, Jewkes R, Martin LJ, Lombard C. The epidemiology of child homicides in South Africa. Bull World Health Organ 2013;91(8):562–8. [CrossRef]
[Pubmed]
5.
Verma SK. Pediatric and adolescent strangulation deaths. J Forensic Leg Med 2007;14(2):61–4. [CrossRef]
[Pubmed]
6.
Sabo RA, Hanigan WC, Flessner K, Rose J, Aaland M. Strangulation injuries in children. Part 1. Clinical analysis. J Trauma 1996;40(1):68–72. [CrossRef]
[Pubmed]
7.
Nixon JW, Kemp AM, Levene S, Sibert JR. Suffocation, choking, and strangulation in childhood in England and Wales: Epidemiology and prevention. Arch Dis Child 1995;72(1):6–10. [CrossRef]
[Pubmed]
8.
Shapiro-Mendoza CK, Kimball M, Tomashek KM, Anderson RN, Blanding S. US infant mortality trends attributable to accidental suffocation and strangulation in bed from 1984 through 2004: Are rates increasing? Pediatrics 2009;123(2):533–9. [CrossRef]
[Pubmed]
9.
Alder C, Polk K. Child Victims of Homicide. Cambridge: Cambridge University Press; 2001.
10.
Hougen HP, Rogde S, Poulsen K. Homicides in two Scandinavian capitals. Am J Forensic Med Pathol 1999;20(3):293–9. [CrossRef]
[Pubmed]
11.
Gupta A, Rani M, Mittal AK, Dikshit PC. A study of homicidal deaths in Delhi. Med Sci Law 2004;44(2):127–32. [CrossRef]
[Pubmed]
12.
Lalwani S, Sharma GASK, Rautji R, Bhardwaj DN, Dogra TD. Pattern of violent asphyxial deaths in south Delhi: A retrospective study. Ind Med Gaz 2004;138:258–61.
13.
Lockemann U, Koops E, Püschel K. Strangulation fatalities in childhood. [Article in German]. Beitr Gerichtl Med 1992;50:13–20.
[Pubmed]
14.
Ghangale AL. Methods of suicidal deaths reported at G.M.C. Nagpur. Int J Med Toxicol Leg Med 2002;4:25–7.
15.
Schoenberg BS, Mellinger JF, Schoenberg DG. Cerebrovascular disease in infants and children: A study of incidence, clinical features, and survival. Neurology 1978;28(8):763–8. [CrossRef]
[Pubmed]
16.
Gastaut H, Pinsard N, Gastaut JL, Regis H, Michel B. Acute hemiplegia in children. Adv Neurol 1979;25:329–37.
[Pubmed]
17.
Fritsch G. Acute infantile hemiplegia caused by cerebral ischemic infarction. Etiology, clinical features and investigations. Padiatr Padol 1984;19(3):287–301.
[Pubmed]
18.
Dooling EC, Richardson EP Jr. Delayed encephalopathy after strangling. Arch Neurol 1976;33(3):196–9. [CrossRef]
[Pubmed]
19.
Bird CR, McMahan JR, Gilles FH, Senac MO, Apthorp JS. Strangulation in child abuse: CT diagnosis. Radiology 1987;163(2):373–5. [CrossRef]
[Pubmed]
20.
Gok E, Cetin S, Baduroglu E, Fedakar R, Akan O, Saka NE. Two accidental hanging cases of children. J Pak Med Assoc 2015;65(7):790–2.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Yakhya Cisse - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Thiam Mbaye - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Faye Mohameth - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bakonde Essosolim - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Barry Lounceny Fatoumata - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Badiane Seydou Boubakar - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Yakhya Cisse et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.