 |
Case Report
Microsurgical neck reconstruction in an elderly patient
1 General Surgery Resident, General Surgery Department, Hospital Ángeles Del Pedregal, Mexico
2 Plastic Surgeon, Plastic Surgery Department, Hospital Ángeles Del Pedregal, Mexico
3 Radiology Resident, Radiology Department, Hospital Ángeles Del Pedregal, Mexico
4 Oncological Surgeon, Oncology Surgery Department, Hospital Ángeles Del Pedregal, Mexico
5 Pediatric Resident, Pediatrics Department, Instituto Nacional de Pediatria, Mexico
6 Microsurgery, Hand Surgeon and Plastic Surgery, Plastic Surgeon, Plastic Surgery Department, Hospital Ángeles Del Pedregal, Mexico
Address correspondence to:
Lopez Mendoza Francisco Javier
Microsurgery, Hand Surgeon and Plastic Surgery, Plastic Surgeon, Plastic Surgery Department, Hospital Ángeles Del Pedregal, Mexico, Camino de Sta. Teresa 1055-S, Héroes de Padierna, La Magdalena Contreras, 10700, Ciudad de México, CDMX,
Mexico
Message to Corresponding Author
Article ID: 100090Z06DM2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Mauricio DCT, Jose TT, Miguel MCY, Javier OCF, Arcelia CDVR, Javier LMF. Microsurgical neck reconstruction in an elderly patient. About a case and review of the literature. Case Rep Int 2021;10:100090Z06DM2021.ABSTRACT
Introduction: The incidence of dermatological malignancies increases with age and a considerable percentage of older adults will require radical surgeries and adjuvant treatments, microsurgery allows repair and coverage of major defects with success rates of up to 90%.
Case Report: We present the case of an elderly patient with an ulcer in the left clavicular region without evidence of healing. Histological and imaging studies were performed, a basal cell carcinoma subtype morphea was found. A wide excision and axillary lymph node dissection were performed, subsequently covering the defect with a free flap. There is an 11-year follow-up.
Conclusion: Complications in microsurgical reconstructions are more associated with comorbidities than with the age of the patient. The same success rates can be obtained in elderly patients.
Keywords: Aged, Basal cell, Microsurgery, Reconstruction
INTRODUCTION
Nowadays human’s life expectancy has increased. Therefore, the percentage of elderly people has increased over the past decade from 5.7% to 29.9% [1],[2]. However, death rate associated with cancer has increased proportionally with age and a significant percentage will require radical surgical procedures in order to achieve free margins [1].
Basal cell carcinoma is the most common type of skin cancer, less than 10% are morphea type. These have aggressive behaviors with local destruction and high local recurrence rate. Lymphatic metastasis are rare, less than 0.005%. The standard treatment is the resection with wide margins and immediate or delayed reconstruction [3].
Historically, it has been considered that age was a contraindication for major surgeries because of the increased death. However, recent improvements in techniques have reduced morbidity and death rates. Thus, allowing major and more complex surgeries in a safer manner [4].
Microsurgery has allowed access to extensive surgeries and complex defects reconstruction. Nowadays flaps are the most popular treatment for complex defects and have reached a success rate above 90%, thus becoming an attractive procedure on the reconstruction field [2],[5].
CASE REPORT
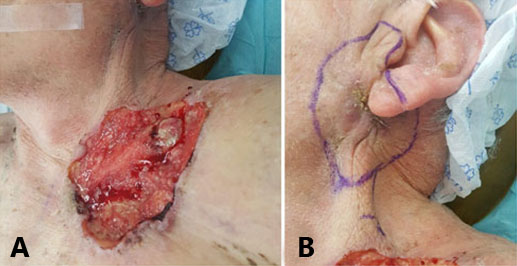
We present the case of an 82-year-old male who arrived with a painless ulcer located on the left supraclavicular region which presented progressive growth over the last 6 weeks (Figure 1A). An ulcerated injury was found on the left supraclavicular region; of approximately 10 × 13 cm2; the edges were erythematous, pearly, and well defined (Figure 1B).
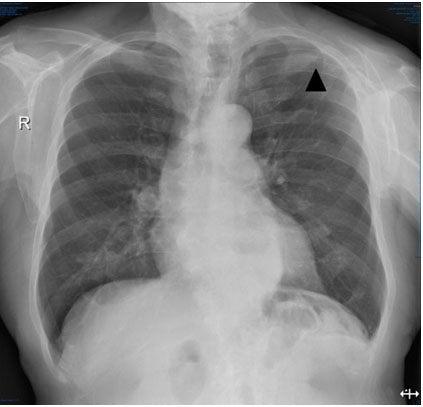
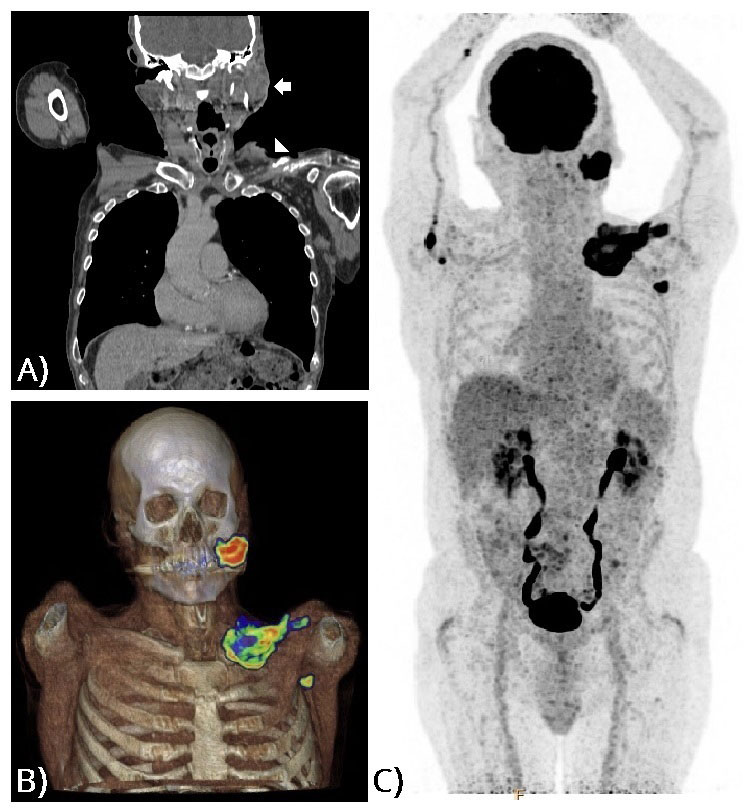
A thorax radiograph (Figure 2) showed a clavicle irregularity among the left edge, suggesting oncological infiltration. A biopsy of the edge and bottom of the injury was performed which resulted in basal cell carcinoma. A positron emission tomography/computed tomography (PET/CT) was requested (Figure 3) in which it was observed that the supraclavicular lesion extended to deep planes. A preauricular lesion was also found, corresponding to a neoplasm in the left parotid region and left axillary adenopathy, all with an increased metabolism. It was classified as a T4N1M0 (Stage IV).
After the above data the need for surgical intervention was decided, American Society of Anesthesiologists (ASA) II risk was assigned. A wide resection was performed in both the lesions (Figure 4) which included left clavicular resection, total left parotidectomy with facial nerve sparing, level II modified radical neck dissection, and a level I axillary dissection.
A 40 × 14 cm defect was reconstructed with a skin flap from rectus abdominis muscles dependent on the deep inferior epigastric artery with a termino-terminal anastomosis to the transverse cervical and a latero-terminal anastomosis to the external jugular under microscope. A 5 × 5 cm deltopectoral graft was used to cover the residual defect in the deltoid zone (Figure 5).
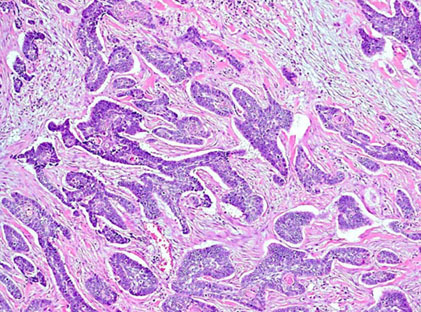
The histological diagnosis (Figure 6) of the supraclavicular and the preauricular lesion was basal cell carcinoma morphea subtype, the margins of the resected tumors were free of disease. The axillary tissue also showed basal cell carcinoma with morphea subtype.
The patient was discharged on the fifth postoperative day. During the postoperative follow-up, there was necrosis of the medial border (approximately 1 × 9 cm) and an island in the deltoid region (3 × 2.4 cm), the probable cause was that these areas were outside the angiosome. The patient required debridement of the injured regions and healing for 2 months until tertiary closure with a full-thickness skin graft (Figure 7A).
The patient completed a hypofractioned radiotherapy scheme in 10 sessions. The 8-months follow-up shows the absence of local and lymph node disease, the flap with adequate vascular permeability and no facial palsy (Figure 7B).



DISCUSSION
Cancer is a prevalent disease in elderly populations, head and neck cancer represents 5% of all cancer reported [4]. Morphea type basal cell skin cancer is an aggressive variant, standard treatment is excision with wide margins and reconstruction of skin defects [3].
The success rate in microvascular procedures in elderly is 95.9% average, the general complication rate is between 17.9% and 22.3% [6],[7]. Surgical complication rates are 20.72% also comparable to younger patients [2],[6],[7],[8] and medical complications are more frequent, occurring in 26.85% of reconstruction [5],[6],[8].
The most widely used skin flaps for defects in head and neck are the anterolateral thigh (ALT), radial forearm, and rectus abdominis [6],[9]. In elderly a large percentage have peripheral arterial disease which diminishes the blood flow of the perforating blood vessels in lower limbs which decreases the performance of the ALT [9].
On this patient, a rectus abdominal flap, an axial flap, was used because of the size of the defect, the perfusion area is 151.6–196.1 cm2. In this flap most complications occur in Zone 4 of Scheflan and Dinner [10].
This patient had an ASA II risk which could have been the reason no major medical complications occurred in the postoperative period. No complications were present in the vascular pedicle and the reason for vascular congestion and necrosis of graft borders was probably due to the size of the graft exceeding the perfusion area of the angiosome.
Complications related to grafts are present in 12.5% of the cases and graft failure in 1.8% [8]. Major complications such as venous thrombosis (63.6%) and arterial thrombosis (3.6%) are present in 10.9% of patients in which 27.8% is rescued in re-exploration [2][4],[5]. The factors associated with surgical complications are ASA ≥ III (odds ratio (OR) 1.62), obesity (OR 1.03), prolonged surgical time (OR 1.0), and hospital stay (OR 1.03) [6],[7].
Significant associations between age and medical complications were found [1],[10]. Major complications were found in 10.7% and minor complications in 44%. The factors that demonstrated independent association are: renal disease (OR 10.13), ASA ≥ III (OR 2.57), and prolonged hospital stay (OR 1.06) [6].
The relationship between age and mortality rate is controversial, Jubbal et al. [6] found that patients in the 6th decade of life have 0.6% mortality, in the 7th decade 1.8%, and that age is associated with 30-day mortality.
CONCLUSION
Physical age and chronologic age may be independent parameters. Currently advanced age is not a contraindication to realize microsurgery. It is associated with an increase in medical complications, but it has the same success rates. Patient selection and perioperative management of comorbidities allow us to realize microsurgery in a safe way in elderly patients.
REFERENCE
1.
Organización Mundial de la Salud. Informe Mundial Sobre el Envejecimiento y la Salud. 1ed. Estados Unidos: Organización Mundial de la Salud; 2015.

2.
Coskunfirat OK, Chen HC, Spanio S, Tang YB. The safety of microvascular free tissue transfer in the elderly population. Plast Reconstr Surg 2005;115(3):771–5. [CrossRef]
[Pubmed]
3.
Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: Epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol 2019;80(2):303–17. [CrossRef]
[Pubmed]
4.
Ferrari S, Copelli C, Bianchi B, et al. Free flaps in elderly patients: outcomes and complications in head and neck reconstruction after oncological resection. J Craniomaxillofac Surg 2013;41(2):167–71. [CrossRef]
[Pubmed]
5.
Özkan Ö, Özgentas HE, Islamoglu K, Boztug N, Bigat Z, Dikici MB. Experiences with microsurgical tissue transfers in elderly patients. Microsurgery 2005;25(5):390–5. [CrossRef]
[Pubmed]
6.
Jubbal K, Zavlin D, Suliman A. The effect of age on microsurgical free flap outcomes: An analysis of 5,951 cases. Microsurgery 2017;37(8):858–64. [CrossRef]
[Pubmed]
7.
Sosin M, Schultz BD, De La Cruz C, Hammond E, et al. Microsurgical scalp reconstruction in the elderly: A systematic review and pooled analysis of the current data. Plast Reconstr Surg 2015;135(3):856–66. [CrossRef]
[Pubmed]
8.
Üstün GG, Aksu AE, Uzun H, Bitik O. The systematic review and meta-analysis of free flap safety in the elderly patients. Microsurgery 2017;37(5):442–50. [CrossRef]
[Pubmed]
9.
Wähmann M, Wähmann M, Henn D, et al. Geriatric patients with free flap reconstruction: A comparative clinical analysis of 256 cases. J Reconstr Microsurg 2020;36(2):127–35. [CrossRef]
[Pubmed]
10.
Tan J, Ohjimi H, Takagi S, Kawakami Y, Eto A. Rezoning free muscle-sparing transverse rectus abdominis myocutaneous flaps based on perforasome groupings and a new understanding of the vascular architecture of the deep inferior epigastric artery-based flaps. Ann Plast Surg 2019;83(6):e59–67. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
De la Concha Tiznado Mauricio - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Telich Tarriba Jose - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Muerrieta Costeño Yehu Miguel - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ochoa Carrillo Francisco Javier - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Cano De la Vega Rosa Arcelia - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lopez Mendoza Francisco Javier - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 De la Concha Tiznado Mauricio et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



