|
Case Report
Acute pancreatitis and hepatitis: A rare presentation of Epstein–Barr virus
1 Assistant Professor, Department of Hospital Medicine Lovelace Medical Center, Albuquerque, New Mexico, USA
2 Assistant Professor, Department of Rheumatology, University of New Mexico, Albuquerque, New Mexico, USA
3 Division of Pulmonary and Critical Care Medicine, Yale-New Haven Bridgeport Hospital, Bridgeport, Connecticut, USA
4 Unity Point Cardiology, Des Monies, Iowa, USA
Address correspondence to:
Sathishkumar Ramalingam
8824 Bernal Ct NE, Albuquerque, New Mexico 87113,
USA
Message to Corresponding Author
Article ID: 100092Z06SR2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ramalingam S, Muruganandam M, Arora H, Gunasekaran K, Padmanabhan P. Acute pancreatitis and hepatitis: A rare presentation of Epstein–Barr virus. Case Rep Int 2021;10:100092Z06SR2021.ABSTRACT
Epstein–Barr virus (EBV) usually causes infectious mononucleosis characterized by fever, tonsillar pharyngitis, and lymphadenopathy. The systemic complication of pancreatitis and hepatitis is a rare complication of EBV.
Keywords: Acute pancreatitis, Epstein–Barr virus, Hepatitis
INTRODUCTION
Epstein–Barr virus is a double-stranded DNA virus that commonly affects children and adolescents. It usually causes infectious mononucleosis, characterized by fever, tonsillar pharyngitis, and lymphadenopathy. The vast majority of cases of infectious mononucleosis are self-limiting. We report a rare case of EBV infection with acute pancreatitis and hepatitis.
CASE REPORT
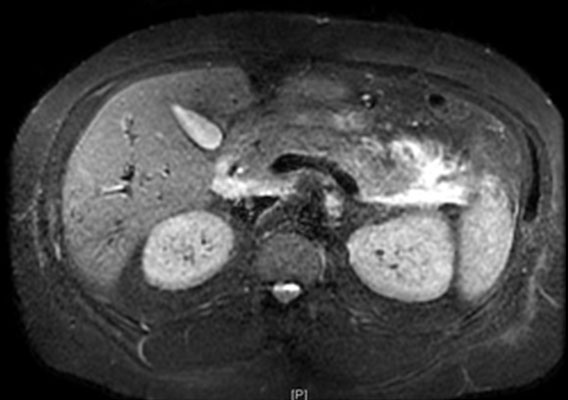
A 31-year-old male with a past medical history of hypertension, attention deficit hyperactivity disorder (ADHD) presented with fever, chills, generalized weakness for a week. He had abdominal discomfort but no sore throat. His temperature was 102.6°F, heart rate 120 per minute, and blood pressure 102/78 mmHg. Laboratory studies were significant for white blood cells 13.3 K/UL, total bilirubin of 8.5 mg/dL, aspartate transaminase (AST) 347 U/L, alanine aminotransferase (ALT) 529 U/L, and alkaline phosphatase of 461 U/L. Ultrasound of the abdomen was unremarkable except for a nonspecific lesion in the right hepatic lobe. His viral hepatitis panel was negative. Infectious mononucleosis assay was positive with both Epstein–Barr virus (EBV) and capsid Ag immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies. Cytomegalovirus (CMV), Coxsackie, mumps, and rubella were negative. His hepatobiliary iminodiacetic acid (HIDA) scan was negative for gallstones. He was a social drinker. He had an abdomen magnetic resonance imaging (MRI) to evaluate hepatic lesion, which showed peripancreatic edema and inflammatory changes consistent with acute pancreatitis (Figure 1). His lipase levels were markedly elevated at 10,683 U/L. He was treated with intravenous fluids, pain medications, and his symptoms resolved. On the tenth day of hospitalization, his lipase was 203 U/L, total bilirubin 3.4 mg/dL, AST 134 U/L, ALT 188 U/L, and his symptoms resolved.
DISCUSSION
Infectious mononucleosis is one of the acute clinical manifestations of Epstein–Barr virus (EBV). Epstein–Barr virus is most common in children, where they are asymptomatic. Infectious mononucleosis is characterized by the triad of fever, tonsillar pharyngitis, and lymphadenopathy, which is usually a mild and self-limiting illness in the adolescent and adults. Epstein–Barr virus has been known to cause hemolytic anemia, thrombocytopenia, hepatitis, splenic ruptures, rash, neurological complications, and various tumors. Similarly, the gastrointestinal system is one of the most common organ systems affected by EBV. Nausea, vomiting, anorexia, and abdominal pain are frequently reported symptoms, probably reflecting mild hepatitis. Abnormal liver functions, including mild elevation of the transaminase, occur in up to 80% of patients with EBV infection. Acute hepatitis with elevated bilirubin is an uncommon presentation of EBV [1].
The most common causes for acute pancreatitis are gallstones, alcohol, medications, infections, and 12% are idiopathic. The most common infectious agents are viruses, which include most commonly mumps, Coxsackie type B, hepatitis B, and CMV. The true incidence of infectious pancreatitis is underestimated as these infections are usually mild or subclinical. Acute pancreatitis due to EBV is an unusual presentation. Only 9 cases have been reported in the literature [2]. Acute hepatitis complicated with pancreatitis usually occurs due to hepatitis A, hepatitis B, or hepatitis E. Acute pancreatitis and cholestatic hepatitis due to EBV is an infrequent presentation. Only 6 cases have been reported in the literature [3],[4]. The diagnosis of EBV pancreatitis is mainly based on serological findings (heterophile antibody test and EBV antibodies), clinical manifestations, imaging tests, and finally, excluding other pancreatitis causes. Most of the patients do well with conservative management.
CONCLUSION
AAcute cholestatic hepatitis and acute pancreatitis are rare complications of EBV. Physicians must be aware of this rare cause, as EBV is one of the most prevalent viruses affecting more than 90% of the population.
REFERENCE
1.
Kang SJ, Yoon KH, Hwang JB. Epstein-Barr virus infection with acute pancreatitis associated with cholestatic hepatitis. Pediatr Gastroenterol Hepatol Nutr 2013;16(1):61–4. [CrossRef]
[Pubmed]

2.
Khawcharoenporn T, Lau WKK, Chokrungvaranon N. Epstein-Barr virus infection with acute pancreatitis. Int J Infect Dis 2008;12(2):227–9. [CrossRef]
[Pubmed]
3.
Mishra A, Saigal S, Gupta R, Sarin SK. Acute pancreatitis associated with viral hepatitis: A report of six cases with review of literature. Am J Gastroenterol 1999;94(8):2292–5. [CrossRef]
[Pubmed]
4.
Galzerano A, Nisi F, Angela S, Ranucci F. Acute Epstein-Barr virus pancreatitis with thoracic-abdominal abscess and portal compression. Dig Liver Dis 2014;46(6):574–5. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Sathishkumar Ramalingam - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maheswari Muruganandam - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Harkesh Arora - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kulothungan Gunasekaran - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Priyesh Padmanabhan - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Sathishkumar Ramalingam et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.