|
Case Report
Syncope: Chief complaint for spontaneous coronary artery dissection without other signs of acute coronary syndrome
1 Mon Health Medical Center, 1200 JD Anderson Drive, Morgantown, WV 26508, USA
Address correspondence to:
Christopher Robert Chew
Mon Health Medical Center, 1200 JD Anderson Drive, Morgantown, WV 26508,
USA
Message to Corresponding Author
Article ID: 100096Z06CC2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Chew CR, Singh A. Syncope: Chief complaint for spontaneous coronary artery dissection without other signs of acute coronary syndrome. Case Rep Int 2021;10:100096Z06CC2021.ABSTRACT
Introduction: Spontaneous coronary artery dissection is an exceptionally rare cause of acute coronary syndrome (ACS) with a reported incidence of 1–4% of all ACS cases. It is most prevalent in young women with the left anterior descending artery and left main are the most common arteries involved.
Case Report: The patient is a 75-year-old man with a prior medical history of hypertension, gastroesophageal reflux disease (GERD), and pulmonary fibrosis presented to the emergency department (ED) with syncope. The patient reported a burning sensation over the central chest different from his GERD. On physical exam, the patient had a 3/6 holosystolic murmur throughout the left pericardium. His laboratory workup was benign with negative troponins and normal electrocardiogram (EKG). Chest X-ray during this time revealed no acute processes and computed tomography angiography (CTA) of the chest was positive for a 4.1 mm fusiform ascending aortic aneurysm. 2D Echo revealed new cardiomyopathy with ejection fraction (EF) of 35–40% with trivial mitral regurgitation (MR) and mild aortic regurgitation. Left heart catheterization revealed left main stenosis of 75%, left anterior descending (LAD) with ostial stenosis of 80% and 30% stenosis of the left circumflex and right coronary artery (RCA). The LAD had a proximal eccentric plaque which under intravascular ultrasound (IVUS) revealed a dissection. The patient underwent a coronary artery bypass grafting (CABG) and did well until discharge home. His postoperative course was complicated by new onset of atrial fibrillation/flutter. The patient was discharged to rehab with Eliquis, baby aspirin, Coreg, and Digoxin.
Conclusion: Our case is unique in view of the unconventional age group, gender, and odd symptomatology. We hope to increase the awareness among medical practitioners for this high morbidity diagnosis if not identified correctly.
Keywords: Asymptomatic, Atherosclerosis, Spontaneous coronary artery dissection
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is a rare cause of ischemic heart disease that is poorly understood. Overall number of cases is reported to be between 1% and 4% of all ACS cases [1]. Most cases reported have occurred in women and approximately 30% of women were peripartum [2]. The rate of SCAD decreases with age with the majority cases under the age of 40 [2]. Men were affected on average younger, 48.6 with a standard deviation of 9.8, versus women at an average age of 52.3 and a standard deviation of 9.2 [3]. Spontaneous coronary artery dissection is most commonly found in the left anterior descending artery [2]. The left main and left anterior descending arteries are more commonly affected in females while the right coronary artery is more common in males [4]. The mainstay for current diagnosis of SCAD has been typically angiography, however, newer technologies such as intravascular ultrasound and optical coherence tomography are being used [2]. As noted by Aziz that a significant number of SCAD cases could be missed by using just angiography alone to identify possible lesions [5]. Intravascular ultrasound or coherence tomography should be used to confirm or rule out a diagnosis [5]. Multidetector computed tomography has been used as follow-up imaging modalities for treated SCAD patients for monitoring [2]. Atherosclerosis is a major cause of SCAD due to plaque rupture leading to a weakened tunica intima and tunica media allowing blood to enter a possible tear. Other causes include connective tissue disorders, fibromuscular dysplasia, and systemic inflammatory conditions [6].
Spontaneous coronary artery dissection is divided into three types. Type one contains a longitudinal filling defect and contains an intimal flap. On angiography, this appears like a double lumen [5]. Type two has diffuse long smooth tubular lesions [4]. There is no visible dissection but rather changes in the arterial diameter between areas that are healthy and lesioned [5]. Type three includes many intramural lesions that appear to be consistent with atherosclerosis [5]. Of the three types, type two is the most common.
A large study of over 750 patients performed by Dr. Jacqueline Saw et al. reported that 70% of patients with SCAD presented with Non-ST-Elevation Myocardial Infarction (NSTEMI) as the most common presenting diagnosis followed by STEMI and ventricular arrhythmias [3]. Troponins were elevated in 97.6% of cases and chest discomfort was the main presenting symptom in 91.5% of cases [3]. A review completed by Hayes et al. determined chest pain was reported in 95.6% of cases as the most common presenting symptom [1]. Majority of the cases in the study were treated conservatively and less than 1% required CABG [5]. The study also followed the patients for 30 days after discharge. It was noted that a recurrent myocardial infarction (MI) occurred in 2.1% of cases, revascularization required in 0.1%, and chest pain reported in 4.9% [3].
CASE REPORT
The patient is a 75-year-old man who presented to the emergency department after having two syncopal episodes over a week’s time which both occurred while the patient was walking. During both instances, the patient lost consciousness but neither time was chest pain reported. In addition to the syncopal episodes, the patient reported a burning sensation over the central chest region. The sensation, however, was reported to be different than his typical gastric reflux symptoms. There were no instigating or relieving factors. There was also a twenty-pound weight loss reported over the past month despite adequate appetite.
The patient’s past medical history is significant for rheumatoid arthritis for which he was taking methotrexate up until the end of 2017 and switched to hydroxychloroquine in 2018. History of deep venous thrombosis (DVT) bilaterally which the patient was on warfarin for chronically. Restrictive lung disease likely secondary to pulmonary fibrosis was also noted. Other chronic issues include hypertension, GERD, and chronic kidney disease III.
Initial labs drawn in the ED were non-contributory. Troponins were drawn twice and remained negative. Vital signs also during admission were within normal limits. Electrocardiogram on admission was non-contributory (Figure 1). Telemetry on admission was normal sinus rhythm.
On physical exam, the patient had a 3/6 holosystolic murmur throughout the left pericardium. Otherwise the patient had a benign physical exam. There was concern for significant mitral regurgitation due to ischemia versus severe aortic stenosis.
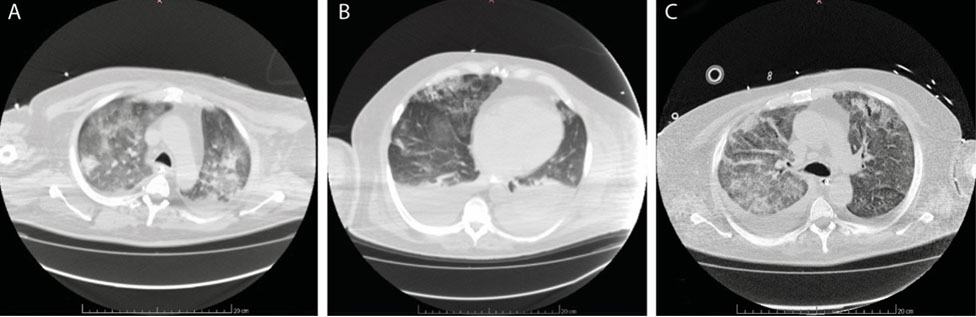
Chest X-ray during this time revealed no acute processes and CTA of the chest was positive for a 4.1 mm fusiform ascending aortic aneurysm that is unassociated with the LAD dissection. Ultrasounds of the carotid arteries bilaterally were negative for stenosis and ultrasounds of the bilateral lower extremities were positive for bilateral DVT.
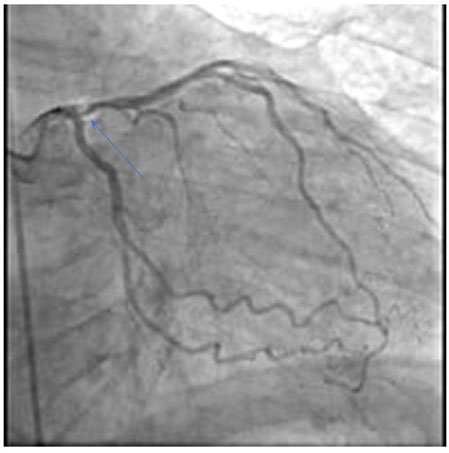
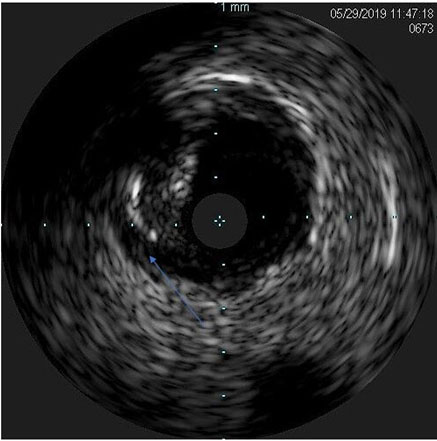
An echo was performed demonstrating an EF of 35–40% and left ventricular hypertrophy (Figure 2). Last echo was from three years prior was benign with an EF of 55–60%. Cardiology was consulted for evaluation following the results of the echo. At the time, cardiology determined a diagnostic heart catheterization was warranted to determine if the cause of the low ejection fraction was due to ischemic versus non-ischemic causes as the patient had no history of congestive heart failure and normal echoes in the past. During the diagnostic catheterization, EF was noted to be 30%. The left main coronary artery had 30–40% ostial disease and a plaque with a cross sectional area of 5.1 mm creating a stenosis of 75%. The left anterior descending coronary artery had a proximal eccentric plaque (Figure 3) which under intravascular ultrasound revealed a dissection (Figure 4). A proximal diagonal artery off the left anterior descending artery had ostial 80% disease. The left circumflex coronary artery and right coronary artery had about 30% stenosis. At this time cardiothoracic surgery was consulted and recommended a CABG be performed because of the patient’s critical multi-vessel disease and dissection. The day before the surgery, the patient was noted to have multiple events of supraventricular tachycardia (SVT) which electrophysiology was consulted for evaluation and clearance for surgery. Heart rates were noted to go as high as 200 beats per minute which terminated spontaneously. The patient did attribute feeling the palpitations during the hospital course and further mentioned they were present during the syncopal episode.
Post-operative complications included hemodynamic instability. The patient developed atrial fibrillation and atrial flutter which was treated with carvedilol and anticoagulated with apixaban. The patient was ultimately discharged fourteen days after admission.


DISCUSSION
This case was presented because of the uniqueness of the patient. The patient had presented to our institution with atypical signs of cardiac etiology for causes of his syncopal episodes. Syncope per literature and case report review has not been noted to be a presenting sign of possible SCAD. The patient did not have elevated troponins which was noted to be elevated in 97.6% patients in one study [3]. Chest pain was also noted to be the primary presenting symptom at 91.6% in the same study [3]. This patient, however, was noted to have very atypical chest discomfort on presentation described as a burning sensation leaning toward a gastric etiology. Also, this patient was a male of elderly age and treated with CABG which conservative management and percutaneous coronary intervention (PCI) being predominantly the treatment of choice. Per one literature review, 50–90% of patients were treated conservatively, 17–47% received PCI, and 2.2–7.4% received CABG [1].
Another case described by Kilic et al. describes a similar case about a 65-year-old man who had an incidental finding of coronary artery dissection [4]. Their patient presented with ST elevations after the start of spinal surgery which at that point he was taken to the CATH lab. He had never complained of angina symptoms in the three years after a previous PCI [4]. Vital signs were noted to be within normal limits and physical exam was benign [4]. During the PCI, the patient was noted to have a lesion in the previously stented region and a non-occlusive spontaneous dissection in the right coronary artery [4]. This patient was treated conservatively and remained symptom free at three and six month follow ups [4].
Recent studies conducted by Kaadan et al. have revealed a possible genetic component involved with the development of SCAD [5]. 44 individuals underwent cardiovascular genetic testing. Of note only 1 of the 44 individuals had a family history of SCAD [5]. Of the 44 individuals, 6 individuals had genetically triggered vascular disease. This included 3 with vascular Ehlers-Danlos syndrome, 1 with nail-patella syndrome, 1 with autosomal dominant polycystic kidney disease, and 1 with Loeys-Deitz syndrome [5]. Conclusion made by their study was that those with positive gene testing are more likely to have SCAD earlier in life.
This case displays the need that cases of syncope warrant a full cardiac workup such as what happened to this patient. Considering this case, the rarity of SCAD, and what has been studied previously shows that there is more that we don’t know as a medical community and the need to further study this rare cause of ACS [7].
CONCLUSION
Spontaneous coronary artery dissection is a relatively rare cause of acute coronary syndrome. If it isn’t diagnosed quickly and treated appropriately, then it can lead to a fatal situation. Not all acute coronary syndromes present as the same and as seen in this case, they can have a rare cause and be relatively asymptomatic.
REFERENCE
1.
Hayes SN, Kim ESH, Saw J, et al. Spontaneous coronary artery dissection: Current state of the science: A scientific statement from the American heart association. Circulation 2018;137(19):e523–57. [CrossRef]
[Pubmed]

2.
Vrints CJM. Spontaneous coronary artery dissection. Heart 2010;96(10):801–8. [CrossRef]
[Pubmed]
3.
Saw J, Starovoytov A, Humphries K, et al. Canadian spontaneous coronary artery dissection cohort study: In-hospital and 30-day outcomes. Eur Heart J 2019;40(15):1188–97. [CrossRef]
[Pubmed]
4.
Kilic ID, Tanriverdi H, Evrengul H, Gur S. A spontaneous coronary artery dissection case noticed during a primary PCI. Cardiol Res Pract 2010;2010:794026. [CrossRef]
[Pubmed]
5.
Aziz S. Spontaneous coronary artery dissection. European Society of Cardiology 2017;14(38).
6.
Almeda FQ, Barkatullah S, Kavinsky CJ. Spontaneous coronary artery dissection. Clin Cardiol 2004;7(7):377–80. [CrossRef]
[Pubmed]
7.
Kaadan MI, MacDonald C, Ponzini F, et al. Prospective cardiovascular genetics evaluation in spontaneous coronary artery dissection. Circ Genom Precis Med 2018;11(4):e001933. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Christopher Robert Chew - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Abhijai Singh - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Christopher R Chew et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.