 |
Case Report
Lady Windermere syndrome: Reality or myth?
1 Resident Physician, Internal Medicine, Piedmont Athens Regional Medical Center, Athens, GA, USA
2 Residnt Physician, Internal Medicine, Piedmont Athens Regional Medical Center, Athens, GA, USA
3 Assistant Professor, Pulmonary and Critical Care, AU/UGA Medical Partnership, Athens Pulmonary and Sleep Medicine, Athens, GA, USA
Address correspondence to:
Prakash Adhikari
MD, 2400 Summerbrook Cir, Unit 2421, Athens, GA 30606,
USA
Message to Corresponding Author
Article ID: 100105Z06PA2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Adhikari P, DaSilva R, Madala N, Fox N. Lady Windermere syndrome: Reality or myth? Case Rep Int 2022;11:100105Z06PA2022.ABSTRACT
Introduction: Mycobacterium avium complex (MAC) is a saprophytic bacterium which can cause pulmonary infection in patients with immunocompromised and structural lung disease. Infection in elderly, non-smoker and healthy women affecting right middle lobe is often referred as Lady Windermere syndrome.
Case Report: We present a case of an 80-year-old woman who presented with progressive worsening shortness of breath and cough and was found to have MAC infection. It is believed that voluntary cough suppression is a possible cause for the colonization and infection by MAC but our patient did not have this habit. Our patient chose not to get treated and she did relatively well without treatment.
Conclusion: Mycobacterium avium complex infection can occur in non-smoker with underlying lung conditions. There are guidelines for management of MAC pulmonary infection with multiple antibiotics and prolonged course and shared decision is recommended prior to initiation of the treatment.
Keywords: Bronchial disease, Bronchiectasis, Mycobacterium avium complex, Mycobacterium infection nontuberculous
INTRODUCTION
In 1987, Prince et al. [1] were the first to describe a series of patients presenting with persistent cough and purulent sputum without weight loss or fever with radiographic pattern of progressive nodular opacities and positive cultures for Mycobacterium avium complex (MAC). In 1992, Reich and Johnson [2] proposed the term Lady Windermere syndrome based upon a review of six individuals with pulmonary disease due to MAC where a distinctive clinical and demographic pattern was featured. All patents were elderly women without clinical evidence of pulmonary disease with inflammatory changes in the lingula and left counterpart lobe without hilar adenopathy or cavitation. The term Lady Windermere refers to a fictional character from Oscar Wilde who portrays a fastidious behavior of cough suppression found in those patients [3].
There is a growing number of evidence that some individuals are predisposed to Lady Windermere syndrome including tall, thin, white elderly women without previous lung disease [3],[4]. However, some reports pointed out male counterparts for this nontuberculous mycobacterial lung disease [5],[6]. In addition, some risk factors have been identified including scoliosis, joint hypermobility, and chest wall pectus abnormalities [3],[4],[7].
In fact, nontuberculous mycobacteria are important pathogens to human and there is evidence of increased prevalence [7], with MAC being the most common species identified in pulmonary disease (4.7 cases per 100,000 persons) [8]. The diagnosis is frequently difficult because MAC is not easily cultured and isolated, and a higher degree of suspicious should be considered in individuals presenting with suggestive symptoms.
CASE REPORT
An 80-year-old woman with history of scoliosis, hypertension, and bronchiectasis in right middle lobe diagnosed four years ago presented to pulmonary clinic with complaint of worsening shortness of breath and productive. The shortness of breath was exertional and was gradually increasing. She used to live independently and performed activities of daily living without any difficulty but recently she started getting short of breath even with these activities. She denied fever, chest pain, and leg swelling. She has never smoked and denied any sick contact. She also denied habit of voluntary cough suppression. She had not travelled out of the states, and she was up to date with vaccination including COVID-19 vaccine. Her cough was productive with production of purulent sputum with no known aggravating or relieving factor. She had no history of weight loss. Her medications were lisinopril 10 mg daily, amlodipine 5 mg daily, and metoprolol 50 mg two times a day for hypertension.
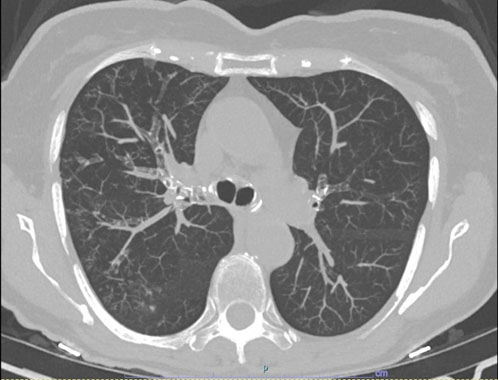
On examination her vitals in the clinic were normal and oxygen saturation was 94% on room air. X-ray chest showed chronic subsegmental atelectasis in the right which was unchanged from previous imaging. Pulmonary function test showed forced expiratory volume at 1 second to forced vital capacity (FEV1/FVC) ratio of 68% with FVC of 55% and FEV1 of 49% predicted indicating obstructive airway disease. The flow volume loop was consistent with the above finding (Figure 1). Computed tomography (CT) scan of chest without contrast was significant for scattered foci of bronchiectasis and tree in bud nodularity within right upper and middle lobe (Figure 2).
Patient underwent bronchoscopy and bronchoalveolar lavage (BAL) was obtained. Preliminary report of the BAL showed no evidence of acid-fast bacilli, fungus, or malignant cell but isolated pseudomonas. The patient was treated with oral levofloxacin for two weeks for pseudomonas. Few weeks later culture isolated M. avium. She was diagnosed with MAC pulmonary infection also known as “Lady Windermere Syndrome” based on her typical features, anatomical location of the involvement, and culture result. The treatment regimen and duration were explained to the patient and her family. They decided not to proceed with the treatment. She came to the clinic three months later for follow up and her symptoms of shortness of breath and cough were somewhat improved.

DISCUSSION
Mycobacterium avium complex pulmonary disease is common in patients with immunocompromised state and pre-existing structural lung disease. Lady Windermere syndrome is MAC pulmonary disease commonly seen in elderly, non-smoker, and relatively healthy women [3]. Radiologically it is different from classic upper lobe fibro-cavitary or nodular bronchiectasis. It is characterized by reticulonodular infiltrates with bronchiectasis involving right middle lobe or lingula [9]. This is a chronic condition and presents with progressive worsening cough with production of purulent sputum and shortness of breath.
Mycobacterium avium complex is a saprophytic bacterium present in soil and water [8]. It can be aerosolized by different means like shower and in normally cleared by mucociliary clearance. There is no human to transmission of MAC [8] . The pathogenesis of Lady Windermere syndrome is not fully understood but different hypotheses have been postulated. The syndrome got its name from the fictional character from Oscar Wilde who portrays a fastidious behavior of cough suppression [2]. Voluntary suppression of cough leading to reduced clearance of secretion from right middle lobe and lingula is one of those proposed mechanism and most of the case reports support this evidence. But many patients also have skeletal abnormalities like scoliosis, pectus excavatum, mitral valve prolapse, or some form of connective tissue disorder [10]. The diminished tensile strength of the airways due to deficit in connective tissue matrix can explain poor clearance of airway and colonization of MAC. In a study by Ismen [10] pectus excavatum, scoliosis, and narrowing of antero-posterior diameter of the chest were significantly high in patient with pulmonary MAC. Our patient fits in this category as she had scoliosis, but no voluntary cough suppression.
Anatomically middle lobe is isolated with poor collateral making re-inflation difficult after development of atelectasis. In addition to that the right middle lobe and the inferior segment of lingula are juxtaposed to the ventricle. Rarefaction and distortion of the lung parenchyma might be contributed by the pulsating heart resulting in disruption in muco-ciliary clearance. Holt et al. [11] proposed immunomodulatory hypothesis for pulmonary MAC in patients with no underlying lung disease. According to their study altered level of adipokines, reduced estrogen, leptin, and ehydroepiandrosterone inhibit macrophage activation and MAC killing.
In another proposed mechanism difference in autonomic balance between men and women due to female hormonal changes could be contributing [4]. A relative reduction in parasympathetic activity in women can cause reduction in mucus production, modify viscoelasticity of the mucus, compromise airway smooth muscle function and decrease respiratory muscle strength, ultimately leading to impaired muco-ciliary clearance and predispose to pulmonary MAC.
Diagnosis of pulmonary MAC can be made by using diagnostic criteria suggested by Infectious Disease Society of America and American Thoracic Society (IDSA/ATS) [12]. But making a diagnosis of MAC disease does not mandate therapy, the decision should be based on weighing the risks and benefits of the treatment and shared decision making is crucial. The therapy recommended by IDSA/ATS statement include three times weekly regimen of clarithromycin or azithromycin, rifampin, and ethambutol for nodular bronchiectasis disease. For fibro-cavitary or severe nodular bronchiectasis daily regimen of above-mentioned medication along with three times weekly amikacin or streptomycin is recommended. Patients should be treated until culture negative on therapy for one year [12].
CONCLUSION
Mycobacterium avium complex pulmonary disease is common not only in immunocompromised patients but also in elderly non-smoker female with underlying lung conditions. Common clinical presentation includes chronic cough, worsening shortness of breath, and weight loss. The mechanism of this condition remains debatable and needs further studies. Diagnosis is based on BAL showing evidence of M. avium in culture. Treatment consists of multiple antibiotics at least for a year and shared decision is recommended prior to initiation of the treatment.
REFERENCE
1.
Prince DS, Peterson DD, Steiner RM, et al. Infection with Mycobacterium avium complex in patients without predisposing conditions. N Engl J Med 1989;321(13):863–8. [CrossRef]
[Pubmed]

2.
Reich JM, Johnson RE. Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest 1992;101(6):1605–9. [CrossRef]
[Pubmed]
3.
Olivier KN. Lady Windermere dissected: More form than fastidious. Ann Am Thorac Soc 2016;13(10):1674–6.
[Pubmed]
4.
Schuh SJ, Dias CF, Schuh GJ, Unis G. Pulmonary disease and the autonomic nervous system: A new pathophysiological mechanism for Lady Windermere syndrome. J Bras Pneumol 2021;47(2):e20200529. [CrossRef]
[Pubmed]
5.
Figueira Gonçalves JM, Rodríguez González J. Lady Windermere syndrome: Does it occur only in women? Arch Bronconeumol 2016;52(10):538–9. [CrossRef]
[Pubmed]
6.
Ku JH, Ranches G, Siegel SAR, Winthrop KL. ‘Lady Windermere’s counterpart? Pulmonary nontuberculous mycobacteria in men with bronchiectasis. Diagn Microbiol Infect Dis 2020;96(2):114916. [CrossRef]
[Pubmed]
7.
Becker KL, Arts P, Jaeger M, et al. MST1R mutation as a genetic cause of Lady Windermere syndrome. Eur Respir J 2017;49(1):1601478. [CrossRef]
[Pubmed]
8.
Cassidy PM, Hedberg K, Saulson A, McNelly E, Winthrop KL. Nontuberculous mycobacterial disease prevalence and risk factors: A changing epidemiology. Clin Infect Dis 2009;49(12):e124–9. [CrossRef]
[Pubmed]
9.
Iseman MD. That’s no lady. Chest 1996;109(5):1411. [CrossRef]
[Pubmed]
10.
Iseman MD, Buschman DL, Ackerson LM. Pectus excavatum and scoliosis. Thoracic anomalies associated with pulmonary disease caused by Mycobacterium avium complex. Am Rev Respir Dis 1991;144(4):914–6. [CrossRef]
[Pubmed]
11.
Holt MR, Miles JJ, Inder WJ, Thomson RM. Exploring immunomodulation by endocrine changes in Lady Windermere syndrome. Clin Exp Immunol 2019;196(1):28–38. [CrossRef]
[Pubmed]
12.
Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007;175(4):367–416. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Prakash Adhikari - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rafael DaSilva - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nikhil Madala - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nik Fox - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Prakash Adhikari et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



