 |
Case Report
Non-inflamed appendix with LAMN causing closed-loop small bowel obstruction
1 Surgical Registrar, Department of General Surgery, Northern Health, Melbourne, Victoria, Australia
2 Surgical Fellow, Department of General Surgery, Northern Health, Melbourne, Victoria, Australia
3 Consultant Surgeon, Department of General Surgery, Northern Health, Melbourne, Victoria, Australia
Address correspondence to:
Hein Maung
Northern Health Hospital, 185 Cooper Street, Epping, VIC 3076,
Australia
Message to Corresponding Author
Article ID: 100122Z06HM2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Maung H, Marino M, Touma F. Non-inflamed appendix with LAMN causing closed-loop small bowel obstruction. Case Rep Int 2023;12(1):17–20.ABSTRACT
Introduction: Low grade appendiceal mucinous neoplasms are generally encountered incidentally in appendicectomies for suspected appendicitis. This case is a documentation of a rare occurrence of LAMN presenting with small bowel obstruction.
Case Report: An 83-year-old male presented to the Emergency Department with a three day history of nausea, vomiting, and obstipation and profoundly dehydrated. Computed tomography revealed a high grade small bowel obstruction with 2 transition points in the right iliac fossa, concerning for closed loop obstruction, necessitating an urgent laparotomy.
Conclusion: While acute appendicitis is a common cause of emergency abdominal pathology, when coupled with small bowel obstruction, a neoplastic cause should be considered as part of the differential diagnosis.
Keywords: Appendicitis, LAMN, SBO
INTRODUCTION
Small bowel obstruction due to an appendiceal inflammation or adhesion is an uncommon presentation, with patients presenting with symptoms of gastrointestinal obstruction, with or without systemic sepsis [1]. Appendicitis causing small bowel obstruction was first described in the literature by Naumov et al. in 1963, and in this case we discuss an even rarer occurrence of this presentation with the additional presence of a low grade mucinous neoplasm [2].
CASE REPORT
An 83-year-old man presented with three days of nausea, vomiting, and obstipation. He had a past surgical history of an open umbilical and inguinal hernia repairs over 10 years prior. He didn’t have any medical comorbidities, and was independent at home with his wife.
On physical examination, he was profoundly dehydrated with decreased skin turgor, pallor, dry mucous membranes and was in rapid atrial fibrillation, with a low blood pressure of 103/60, and afebrile. His abdomen was distended, tympanic, and was generally tender.
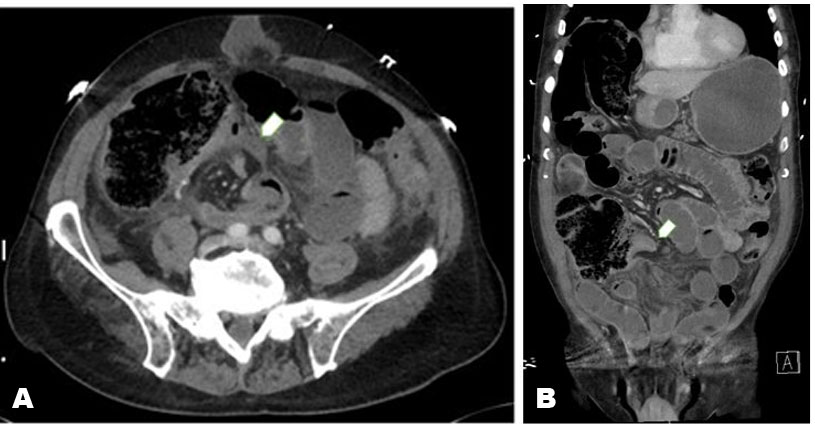
Hemoglobin was 11.3 g/dL; white blood cell count was 14.5 × 109/L; C-reactive protein was 98 mg/dL; Creatinine 170 umol/L. Computed tomography (CT) of his abdomen demonstrated a high-grade small bowel obstruction (SBO) with two transition points within the right iliac fossa. The intervening bowel was edematous, concerning for an ischemic closed loop.
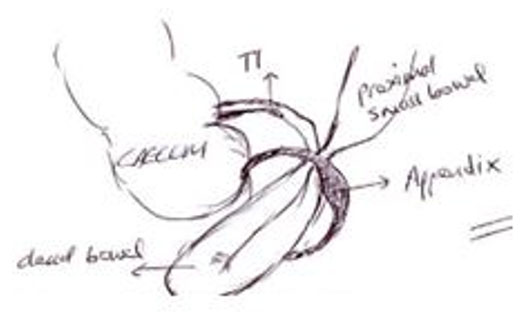
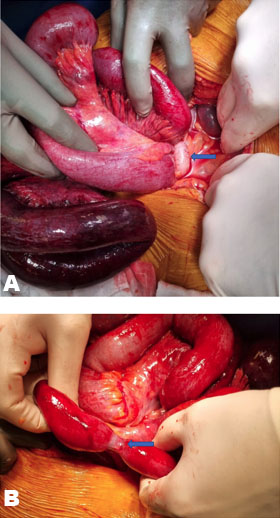
A nasogastric (NG) tube was inserted for draining copious amounts of bilious fluid over 1 liter, and he was resuscitated in the emergency department (ED) prior to the operating theater for an emergency laparotomy. Turbid free fluid was found on entry. A 50-centimeter loop of ischemic, non-viable small bowel was found incarcerated underneath a ring formed by the appendix 15-centimeters from the terminal ileum, forming a closed-loop SBO. The appendix was non-inflamed and had a prominent thickening in its mid-portion, the tip of which was embedded within the mesentery of the terminal ileum. The band was released and appendectomy performed. The ischemic small bowel was resected and a stapled side to side anastomosis performed. The patient made an uneventful recovery and was discharged post-operative day 7.
Histology revealed a low-grade mucinous neoplasm (LAMN) within the mid-portion of the appendix over 1-centimeter from the nearest margin, with no invasive component and no perforation or extravasated mucin. The patient was discussed at a multidisciplinary team meeting where it was deemed no further treatment was necessary (Figure 1, Figure 2, Figure 3).
DISCUSSION
Small bowel obstructions are a common cause of surgical admission. The most common causes of SBO are adhesional, accounting for 75% of all SBO [3]. The appendix as a cause of SBO has now been well reported in the literature; however, almost exclusively in the context of appendicitis [4],[5],[6]. An “appendiceal tie” strangulating the small bowel via appendicitis has been documented in the literature and was first described by in 1963 [2],[5],[7]. A classification system for SBO in the context of appendicitis has been suggested, with mechanisms via adynamic (paralytic ileus), mechanical without strangulation, strangulation, and finally mesenteric ischemia [8]. A literature review in 2017 by Makama et al. identified 45 patients with obstruction due to appendicitis: (A) Appendix laid across bowel loops bound by adhesions; (B) Herniation through a ring or gap formed by appendix tip attached to base; (C) Tip attached to bowel causing torsion; (D) Kinking of bowel; (E) Complex knotting [1].
In our case, SBO was caused by the mechanism of strangulation with the tip of the appendix embedded in the mesentery of small bowel, forming a “ring” for small bowel to herniate through. The underlying cause of the adhesion is speculated to more likely have been secondary to previous tip appendicitis rather than the LAMN itself, given its location—the LAMN was mid appendix, while the tip was embedded in the mesentery of the ileum, without any signs of acute inflammation.
Low-grade mucinous neoplasm of the appendix is different from most malignant tumors, with a mechanism of growth with a pushing margin of low-grade dysplasia, in contrast to infiltrative growth, and disseminates via perforation leading to pseudomyxoma peritonei (PMP). Two distinct clinicopathological types of LAMN lesions were identified, with type 1 lesions confined to the appendiceal lumen, while type 2 lesions involved appendiceal wall or peri-appendiceal tissue with or without perforation of the appendix, and thus were more likely to be referred for hyperthermic intraperitoneal chemotherapy (HIPEC).
A literature search on PubMed identified 4 cases of appendiceal LAMN causing SBO via adhesions in different locations:
(1) Small bowel mesentery to small bowel mesentery causing partial obstruction,
(2) Ileocecal intussusception,
(3) Adhesions from appendix to small bowel +/− spread of mucin/nodules to peritoneum [3].
In this case, the appendiceal tip had embedded in mesentery without perforation, inflammation, or high-grade features of LAMN. This case would make it a total of 6 documented cases of this rare pathology.
CONCLUSION
While acute appendicitis is a common cause of emergency abdominal pathology, when coupled with small bowel obstruction, a neoplastic cause should be considered as part of the differential diagnosis.
REFERENCE
1.
Cappell MS, Batke M. Mechanical obstruction of the small bowel and colon. Med Clin North Am 2008;92(3):575–97, viii. [CrossRef]
[Pubmed]

2.
Karlsen EA, Mulholland P, Mouline O, Cross T. Appendicular ring: An unusual cause of mechanical small bowel obstruction. ANZ J Surg 2021;91(11):E727–8. [CrossRef]
[Pubmed]
3.
Chowdary PB, Shivashankar SC, Gangappa RB, Varghese EV. Appendicular tourniquet: A cause of intestinal obstruction. J Clin Diagn Res 2016;10(5):PD09–11. [CrossRef]
[Pubmed]
4.
Lawani I, Houndje CYP, Souaïbou YI, et al. Internal hernia strangulated on appendicular tourniquet: A case report of an exceptional anomaly of the appendix revealed by a rare hernia. Surg Case Rep 2019;5(1):112. [CrossRef]
[Pubmed]
5.
Bhandari L, Mohandas P. Appendicitis as a cause of intestinal strangulation: A case report and review. World J Emerg Surg 2009;4:34. [CrossRef]
[Pubmed]
6.
Donovan A, Tabone R, Yuide PJ, Chua TC. Small bowel obstruction from an appendiceal tie. ANZ J Surg 2020;90(9):1796–8. [CrossRef]
[Pubmed]
7.
Samuk I, Dlugy E, Seguier-Lipszyc E, Rootman MS, Nica A, Kravarusic D. Not only appendicitis: Rare appendix disorders manifesting as surgical emergencies in children. Eur J Pediatr 2021;180(2):407–13. [CrossRef]
[Pubmed]
8.
Toh BC, Soh LS, Chew MH. Unusual cause of small intestinal obstruction. ANZ J Surg 2020;90(4):E71–2. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Hein Maung - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Matthew Marino - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fidel Touma - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Hein Maung et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



