|
Case Report
Postpartum intracerebral hemorrhage unveiling moyamoya disease: A rare case report
1 Resident, Radiology Department, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco
2 Professor, Radiology Department, Ibn Sina University Hospital, Mohamed V University, Rabat, Morocco
Address correspondence to:
Merbouh Sahar
Resident, Radiology Department, Ibn Sina University Hospital, Mohamed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 100123Z06MS2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sahar M, Ilyass B, Cherraqi A, Zahra LF. Postpartum intracerebral hemorrhage unveiling moyamoya disease: A rare case report. Case Rep Int 2023;12(2):21–25.ABSTRACT
Moyamoya disease (MMD) is an uncommon cerebrovascular disorder characterized by abnormal angiogenesis leading to progressive stenosis of the supraclinoid internal carotid artery. The resultant vascular pathology causes the formation of a compensatory collateral network, often visualized as a characteristic “puff of smoke” appearance on imaging. This report aims to present the case of a 36-year-old female patient who presented with altered consciousness and left hemiparesis two weeks after undergoing a cesarean section delivery, with moyamoya disease identified as the underlying cause of the stroke. The objective is to underscore the importance of considering moyamoya disease as a potential etiology in postpartum stroke cases and emphasize the significance of early diagnosis and appropriate management to improve patient outcomes. Timely imaging and appropriate treatment, such as revascularization surgery, can help prevent further neurological deterioration and potentially improve long-term prognosis for these patients.
Keywords: Angiography, Intracerebral hemorrhage, Moyamoya disease, Puff of smoke, Stroke
INTRODUCTION
Moyamoya disease is an angiogenic disorder characterized by stenosis of the distal portion of the internal carotid artery and the proximal portion of the middle and anterior cerebral arteries. It is associated with the development of an irregular replacement vascular supply network. These vessels are pathologic, fragile, and may present dilations and microaneurysms, which increase the risk of intracerebral and/or ventricular hemorrhage [1]. Hemorrhagic manifestations are more common in adults, whereas ischemic manifestations are more frequent in children [2]. The etiology of moyamoya disease remains poorly understood.
CASE REPORT
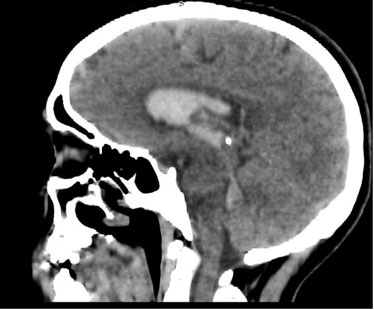
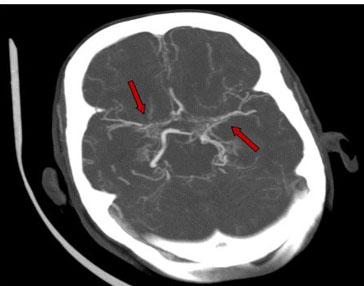
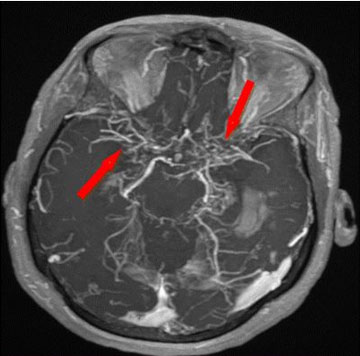
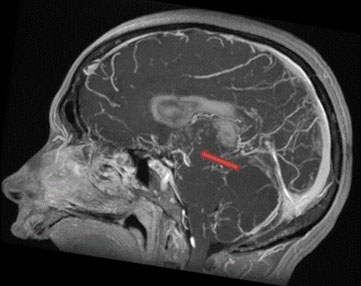
A 36-year-old woman primipara gravida I, para 1 with no medical history presented to the emergency department with altered consciousness and hemiparesis two weeks following a cesarean delivery. The patient did not experience any uncontrolled blood pressure issues or pre-eclampsia during her pregnancy or postpartum period. Physical examination revealed blood pressure of 150/100 mm, an isolated sensory and motor deficit on the left side of the body. A brain computed tomography (CT) scan was performed which demonstrated intraventricular hemorrhage (Figure 1), ANGIO CT revealed stenoses in the proximal segments of the bilateral middle cerebral arteries and the left posterior cerebral artery surrounded by small abnormal net-like vessels of collateral circulation (Figure 2). Magnetic resonance imaging was performed as part of the etiological assessment revealing intraventricular hemorrhage with T1 hypersignal and blooming in magnetic resonance susceptibility-weighted imaging (SWI). Magnetic resonance angiography (MRA) demonstrated stenoses and occlusions in the proximal segments of the bilateral middle cerebral arteries and the left posterior cerebral artery (Figure 3 and Figure 4), accompanied by a compensatory collateral vascular network recanalizing the distal segments, resulting in a characteristic “puff of smoke” appearance (Figure 5).

DISCUSSION
Moyamoya is a Japanese word that translates to a puff of cigarette smoke floating in the air [3]. Moyamoya disease is an idiopathic vascular occlusive disorder that predisposes affected patients to strokes due to progressive stenosis of the intracranial internal carotid arteries and their proximal branches [4]. The etiology of the disease is still poorly understood and the pathogenesis is not well known, it suggests an idiopathic origin that most likely involves both genetic and environmental factors. The progressive thickening of the cerebral artery walls causes reduced blood flow in the major vessels of the brain’s anterior circulation, leading to the production of angiogenic factors responsible for the formation of replacement collateral neovessels. These neovessels form through various pathways, including the intraparenchymal perforating arteries, the leptomeningeal collaterals of the posterior cerebral artery, the trans-dural collaterals of the middle meningeal artery, the superficial temporal artery, the ethmoidal artery and/or the occipital artery [1].
Many factors, including hemodynamic, hormonal, and pharmacological changes during pregnancy and the post-partum period, increase the risk of stroke. Progesterone has been implicated in promoting a hypercoagulable state in pregnant women, making them more susceptible to thrombosis. Increased levels of progesterone have been associated with changes in clotting factors, such as increased fibrinogen levels and decreased antithrombin III activity, leading to a prothrombotic state. This hypercoagulable condition is considered a protective mechanism to prevent excessive bleeding during childbirth but can also predispose pregnant women to thromboembolic events, including strokes. In the context of moyamoya disease, the progressive narrowing and occlusion of cerebral arteries already compromise blood flow to the brain. The additional thrombogenic effect of pregnancy hormones may exacerbate the situation, increasing the risk of stroke in pregnant women with undiagnosed or known MMD [5].
The exact prevalence of moyamoya disease varies in different populations and regions, but it is generally considered to be a rare cerebrovascular disorder. The incidence and prevalence of moyamoya disease may be higher in certain patient populations or races, particularly in individuals of Asian descent, compared to other ethnic groups [6]. Moyamoya disease can lead to both cerebral ischemia and hemorrhage including intracerebral, intraventricular, and subarachnoid hemorrhage. The common site of hemorrhage is intraventricular as observed in our case. Clinical manifestations of the disease vary, with transient or persistent ischemic strokes being more common in the pediatric population, while hemorrhagic strokes are predominant in young adults [7]. In children with moyamoya disease the majority experience transient ischemic attacks (TIA) characterized by symptoms such as hemiparesis, monoparesis, and sensory disturbances, as well as cerebral infarction. In adult patients, approximately half develop intracranial hemorrhage, while the other half experience TIA or cerebral infarction [8],[9].
Our patient was a previously unknown case of moyamoya and experienced intraventricular hemorrhage two weeks after giving birth. There is limited scientific data available on the assessment of complications associated with moyamoya angiopathy during pregnancy and the peripartum period. Until delivery, there doesn’t appear to be a significant increase in cerebrovascular complications. However, in the peri- and postpartum period, reported complications such as cerebral hemorrhage and transient ischemic attack mostly involve patients who were not previously diagnosed with moyamoya angiopathy, similar to our patient’s case [10].
Computed tomography imaging can reveal signs of ischemic or hemorrhagic stroke. On the other hand, ANGIO CT can provide detailed information about stenoses and occlusions of the internal carotid arteries and/or the proximal segments of the anterior and middle cerebral arteries. It enables visualization of the collateral vascular network as small abnormal net-like vessels located at the site of the circle of Willis.
Magnetic resonance imaging and magnetic resonance angiography
Magnetic resonance imaging and MRA can be performed as a first-line procedure for evaluating moyamoya disease. They have a sensitivity and specificity ranging from 70% to 100% [1]. Conventional sequences will be useful for demonstrating parenchymal complications. Ischemic lesions will appear as a T1 hypointense signal, T2 hyperintense signal, FLAIR signal, and diffusion signal varies depending on the age of the lesion. Hemorrhagic lesions will exhibit variable signals in T1 and T2 sequences depending on the age of the hemorrhage, while consistently showing a T2* hypointense signal [11].
Conventional cerebral angiography remains the gold standard imaging technique for suspected moyamoya disease due to its excellent spatial resolution. It can effectively demonstrate the characteristic features of chronic steno-occlusive angiopathy, affecting primarily the supraclinoid internal carotid arteries (ICAs) and the proximal anterior and middle cerebral arteries (ACAs/MCAs). Additionally, it enables the identification of microaneurysms, which can be a source of cerebral hemorrhage and may not always be detectable with other imaging modalities. Moyamoya disease is often suggested by several factors, including the patient’s younger age, the presence of bilateral/symmetrical lesions, and the pattern of arterial collateralization. A prominent collateral vascular network, characterized by neoangiogenesis around the circle of Willis, which is responsible for the distinctive “puff of smoke” sign often observed in MMD cases [12],[13].
Some other conditions can present images that are very similar to those of moyamoya disease. Steno-occlusive lesions at the bifurcation of carotid arteries may be observed without an associated neovascular network. In such cases, a differential diagnosis should be considered, including reversible cerebral vasoconstriction syndrome, intracranial atheroma, intracranial dissection, primary central nervous system vasculitis, and transient cerebral arteriopathy in childhood [10].
Patients who have well-known associated risk factors or underlying conditions are diagnosed with moyamoya syndrome, while patients without any known associated risk factors are diagnosed with moyamoya disease. The pathognomonic arteriographic findings are typically bilateral in moyamoya disease. However, patients with unilateral findings are still classified as having moyamoya syndrome, even if they do not have any other associated risk factors. It is important to note that in up to 40% of patients initially presenting with unilateral findings, contralateral disease eventually develops over time [4].
There is currently no medical treatment available to stabilize the progression of the disease. Surgical revascularization is considered the most effective therapy for improving cerebral hemodynamics and reducing the risk of future strokes. Both direct and indirect bypass surgeries can help improve the compromised cerebral circulation and alleviate clinical symptoms [9],[14].
CONCLUSION
Moyamoya disease is a rare chronic intracranial arteriopathy of undetermined origin. The most common clinical manifestation is a sequence of ischemic or hemorrhagic events without conventional risk factors. Angioscanning and angioMR are currently the standard imaging modalities for initial diagnosis and monitoring. Arteriography remains the gold standard for precise assessment of lesions and definitive diagnosis.
REFERENCE
1.
Chibli R, Omor Y, Sebbouba NS, Hassani MRE, Jiddane M, Fikri M. Moya moya disease: A rare cause of ischemic stroke in children: About a case. [Article in French]. Pan Afr Med J 2017;28:192. [CrossRef]
[Pubmed]

2.
Nassaf M, Draiss G, Rada N, Bourrous M, Bouskraoui M. Moyamoya disease in children: A case report. [Article in French]. Arch Pediatr 2012;19(5):493–6. [CrossRef]
[Pubmed]
3.
Takeuchi S, Kobayashi K, Tsuchida T, Imamura H, Tanaka R, Ito J. Computed tomography in moyamoya disease. J Comput Assist Tomogr 1982;6(1):24–32. [CrossRef]
[Pubmed]
4.
Scott RM, Smith ER. Moyamoya disease and moyamoya syndrome. N Engl J Med 2009;360(12):1226–37. [CrossRef]
[Pubmed]
5.
Liu XJ, Zhang D, Wang S, et al. Intracranial hemorrhage from moyamoya disease during pregnancy and puerperium. Int J Gynaecol Obstet 2014;125(2):150–3. [CrossRef]
[Pubmed]
6.
Kuriyama S, Kusaka Y, Fujimura M, et al. Prevalence and clinicoepidemiological features of moyamoya disease in Japan: Findings from a nationwide epidemiological survey. Stroke 2008;39(1):42–7. [CrossRef]
[Pubmed]
7.
Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis; Health Labour Sciences Research Grant for Research on Measures for Infractable Diseases. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo) 2012;52(5):245–66. [CrossRef]
[Pubmed]
8.
Kuroda S, Houkin K. Moyamoya disease: Current concepts and future perspectives. Lancet Neurol 2008;7(11):1056–66. [CrossRef]
[Pubmed]
9.
Fukui M, Kono S, Sueishi K, Ikezaki K. Moyamoya disease. Neuropathology 2000;20 Suppl:S61–4. [CrossRef]
[Pubmed]
10.
MPR pédiatrique, Hôpital Bellevue, Maladie et syndrome de moyamoya de l’enfant et de l’adulte. CHU de Saint Etienne. Paris: Centre de référence des maladies vasculaires rares du cerveau et de l’oeil (CERVCO), 2016. p.12–3.
11.
Kikuta K, Takagi Y, Nozaki K, et al. Asymptomatic microbleeds in moyamoya disease: T2*-weighted gradient-echo magnetic resonance imaging study. J Neurosurg 2005;102(3):470–5. [CrossRef]
[Pubmed]
12.
Yoon HK, Shin HJ, Lee M, Byun HS, Na DG, Han BK. MR angiography of moyamoya disease before and after encephaloduroarteriosynangiosis. AJR Am J Roentgenol 2000;174(1):195–200. [CrossRef]
[Pubmed]
13.
Burke GM, Burke AM, Sherma AK, Hurley MC, Batjer HH, Bendok BR. Moyamoya disease: A summary. Neurosurg Focus 2009;26(4):E11. [CrossRef]
[Pubmed]
14.
Mesiwala AH, Sviri G, Fatemi N, Britz GW, Newell DW. Long-term outcome of superficial temporal artery-middle cerebral artery bypass for patients with moyamoya disease in the US. Neurosurg Focus 2008;24(2):E15. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgement
The authors thank Professor Fatima Zahra Laamrani insight vis-à-vis the case.
Author ContributionsMerbouh Sahar - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bourekba Ilyass - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amine Cherraqi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Laamrani Fatima Zahra - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Merbouh Sahar et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.