|
Case Report
Emergent use of a central venous catheter placed in the internal mammary vein
1 Resident Physician, Internal Medicine, University of North Carolina, Chapel Hill, North Carolina, United States
2 Professor, Division of Pulmonology and Critical Care, University of North Carolina, Chapel Hill, North Carolina, United States
Address correspondence to:
Richard Jensen
MD, 126 MacNider Hall, Campus Box #7005, Chapel Hill, North Carolina,
United States
Message to Corresponding Author
Article ID: 100127Z06RJ2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Jensen R, Henderson AG. Emergent use of a central venous catheter placed in the internal mammary vein. Case Rep Int 2024;13(1):12–15.ABSTRACT
Introduction: Central venous catheter (CVC) insertion plays an important role in critical care medicine, often utilized for vasopressor administration, volume resuscitation, reliable venous access, and central venous pressure monitoring. However, there are potential complications associated with placement, including arterial cannulation, catheter fragmentation, venous injury, pneumothorax, and malposition into a tributary vessel.
Case Report: A 35-year-old woman with a history of severe psoriasis with recurrent superinfection, and right internal jugular (RIJ) venous thrombosis was transferred to the intensive care unit with septic shock. A CVC was inserted via left internal jugular (LIJ) to facilitate antimicrobial administration and continued vasopressor support, as it was patent by bedside ultrasound. The patient was asymptomatic during and after CVC placement. However, post-procedure chest X-ray demonstrated a CVC projecting directly inferiorly, ending over the left hemidiaphragm. After review of recent cross-sectional imaging, physical examination, blood gas assessment, and ultrasound evaluation, the catheter was thought to be within the internal mammary vein (IMV). Given the patient’s instability and being asymptomatic after line placement with the CVC functioning normally, the decision was made to temporarily use the line. The next day, its placement was confirmed by using computed tomography (CT).
Conclusion: Miscannulation of a tributary vessel during CVC placement can cause significant morbidity and even mortality. However, it has been postulated that a line placed within the IMV could be used safely in the emergent setting. Our case demonstrates the safe utilization of a CVC within the IMV and provides a reasonable framework for approaching a misplaced LIJ CVC.
Keywords: Central line, Central venous catheterization, Internal mammary vein, Miscannulation
INTRODUCTION
Central venous catheter (CVC) insertion plays an important role in critical care medicine, with common indications being vasopressor administration, volume resuscitation, the need for reliable venous access, and to monitor central venous pressure. While central venous cannulation is routine, it is accompanied by potential mechanical complications, including arterial cannulation, catheter fragmentation, venous injury, pneumothorax, hemothorax, and malposition into tributary vessels [1],[2]. Here, we present a unique case where left internal jugular (LIJ) vein catheterization inadvertently resulted in cannulation of the internal mammary vein (IMV). Due to patient-specific factors and clinical instability, the line was utilized, a scenario that has only been documented in the literature only once before, more than twenty years ago.
CASE REPORT
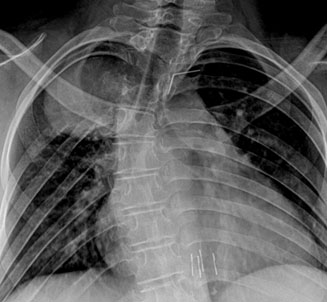
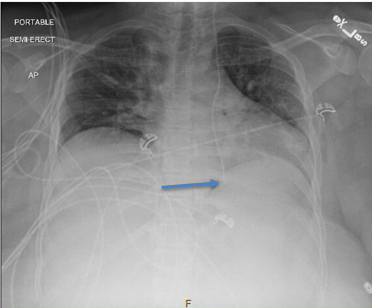
A 35-year-old woman with a history of severe erythrodermic psoriasis on immunosuppression with recurrent superinfection, heart failure with reduced ejection fraction, obesity [body mass index (BMI) 53], and right internal jugular (RIJ) venous thrombosis was transferred to the medical intensive care unit for vasopressor administration and volume resuscitation in the setting of septic shock. On arrival, she presented with sinus tachycardia (123 bpm), hypotension (97/56 mmHg) despite vasopressor support (norepinephrine 14 mcg/min, vasopressin 0.03 units/min), and tachypnea (30 breaths/min). Laboratory findings revealed a new white blood cell count of 51,300 cells per cubic millimeter, increased from 10,700 cells per cubic millimeter previously. Antimicrobial coverage was broadened empirically given her immunocompromised state and history of infection with multidrug-resistant organisms. The decision was made to pursue central venous catheter insertion to facilitate antimicrobial administration and continued vasopressor support. The LIJ vein site was chosen given her known RIJ thrombus, skin infections with severe skin sloughing at both groin sites, and lack of operator experience in subclavian line placement. The LIJ vein site was identified, the area was prepped and draped in usual sterile fashion, and after applying local anesthesia with 1% lidocaine, the wire introducer was inserted into the LIJ using ultrasound guidance. The wire was imaged by ultrasound and properly positioned in the vein prior to dilation. Using the Seldinger technique, a Triple Lumen was placed passing without resistance, each port easily flushed and freely drawing venous blood. Per protocol, a post-procedure chest X-ray was obtained, which demonstrated “Left approach central venous catheter with tubing projecting over the mid portion of the heart and tip projecting at the level of the left hemidiaphragm. Location the catheter is indeterminate; however arterial placement cannot be excluded. The catheter could also be within a venous collateral or internal mammary vein” (Figure 1). Venous blood gases were obtained from two of the three ports, and pressures were transduced, all consistent with venous placement. After discussion with radiology and beside ultrasound evaluation, the decision was made to continue using the line for administration of vasopressors and antibiotics. The following day, a non-contrasted CT scan of the chest confirmed placement of the triple lumen catheter within the IMV (Figure 2). The patient improved and was weaned from vasopressors; the central line was used for approximately 30 hours after placement without complication.

DISCUSSION
The LIJ approach poses an increased risk for anomalous venous cannulation due to the oblique angle of the left innominate vein and its tributaries, including the IMV. Patient-specific factors, such as portal hypertension, anomalous venous drainage, prior vascular surgeries, and tumors, further increase this risk [3]. Misplacement into the IMV is suboptimal and may lead to complications, such as laceration and hemothorax [4]. Early signs, such as resistance to guidewire advancement, inability to aspirate blood, and chest pain, should prompt immediate evaluation as they may indicate complicated line placement [3],[5]. Though the patient did not exhibit symptoms, our initial radiograph prompted consideration of a broad differential including arterial placement, mediastinal perforation, pneumothorax, or anomalous venous placement.
Through clinical reasoning and discussion with our radiology colleagues, we assessed the likelihood of dangerous line misplacement to be quite low. Mediastinal perforation was deemed unlikely due to normal catheter function and the patient’s asymptomatic state post line-placement. Similarly, arterial puncture was ruled out through venous blood gasses and pressure transduction. We were fortunate to have recent cross-sectional chest imaging, which ruled out other anomalous venous drainage. Additionally, the possibility of pericardiophrenic vein placement, known for its potential complication of pericardial tamponade [6], was considered highly improbable, as the catheter passed below the diaphragm on portable chest radiographs. Bedside ultrasound confirmed the absence of any new pericardial or pleural effusion accumulation.
When line misplacement occurs, options include placement at another venous access site or withdrawing and rewiring the sheath under fluoroscopy as a salvage approach [3]. However, it has also been suggested that under emergent circumstances, a catheter placed in the IMV could be safely used for medication administration, supported by fluoroscopic studies demonstrating contrast return to the right atrium and consistent CVP measurements with the superior vena cava [5],[7],[8]. Multidisciplinary discussions between radiology and critical care medicine led us to temporarily utilize the line, considering low risk of other locations of misplacement. Our report underscores the enduring risks associated with line placement and demonstrates a reasonable approach to a misplaced LIJ approach central venous catheter.
CONCLUSION
Our case provides validation to the theory that under emergent circumstances, a catheter placed in the IMV can be safely used for the administration of medications. However, such an approach should only be adopted when extenuating circumstances are present and necessitates multidisciplinary collaboration to appropriately weigh risks and benefits.
REFERENCE
1.
Bowdle A. Vascular complications of central venous catheter placement: Evidence-based methods for prevention and treatment. J Cardiothorac Vasc Anesth 2014;28(2):358–68. [CrossRef]
[Pubmed]

2.
Tashjian BC, Schoor ME, Grant M. Cannulation of the internal mammary vein with a single-lumen infusion catheter in a patient with portal hypertension: A case report. A A Pract 2019;12(4):122–4. [CrossRef]
[Pubmed]
3.
House LM 2nd, Yen A, Bokoch MP. Central venous catheter in the internal mammary vein. Anesthesiology 2019;131(2):397. [CrossRef]
[Pubmed]
4.
Kela M, Munde H, Raut S. Accidental placement of central venous catheter into internal mammary vein: A rare catheter malposition. Ann Card Anaesth 2017;20(4):477–8. [CrossRef]
[Pubmed]
5.
Goodin P, Jain N, Jeelani HM, Bharat A. Accidental central venous catheter placement in the internal thoracic vein: A case report. Cureus 2020;12(7):e9255. [CrossRef]
[Pubmed]
6.
Zaman MH, Mitra P, Bondi E, Gintautas J, Abadir AR. A rare malposition of the central venous catheter. Chest 1990;98(3):768–70. [CrossRef]
[Pubmed]
7.
Sandroni C, Pirronti T, Tortora F, Santangelo S, Rinaldi P, Antonelli M. Unusual central venous catheter malposition into the left internal mammary vein: A case report. Intensive Care Med 2003;29(12):2338–9. [CrossRef]
[Pubmed]
8.
Quigley RG, Petty C, Tobin G. Unusual placement of a central venous catheter via the internal jugular vein. Anesth Analg 1974;53(3):478. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Richard Jensen - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ashley G Henderson - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Richard Jensen et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.