|
Case Report
Syngnathia of the anterior mandible in a newborn: Case report
1 DDS, MD, Oral and Maxillofacial Surgeon, Private Practice, Santa Barbara Facial Reconstruction, Santa Barbara, CA, United States
2 DDS, MS, FACS, Cleft and Craniofacial Oral Surgeon, Carolinas Center for Oral and Facial Surgery, Department of Craniomaxillofacial Surgery, Novant Health Presbyterian Medical Center, Charlotte, NC, United States
Address correspondence to:
Matthew Dailey
334 S. Patterson Ave, Suite 205, Santa Barbara 93111, CA,
USA
Message to Corresponding Author
Article ID: 100131Z06MD2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Dailey M, Kapitan R. Syngnathia of the anterior mandible in a newborn: Case report. Case Rep Int 2025;14(1):6–9.ABSTRACT
Introduction: Congenital maxillomandibular fusion is a rare disorder of the craniomaxillofacial skeleton and soft tissue that may present as fusion of the soft tissue, also known as synechiae, or as bony fusion, also known as syngnathia. True maxillomandibular fusion without the involvement of other craniomaxillofacial structures is an uncommon condition with few occurrences documented.
Case Report: We present the case of a newborn infant with intra-utero documented absence of the second through fourth digits on the right hand and micrognathia visualized on ultrasound. No specific syngnathia or cleft lip or palate was noted. At birth he had congenital malformations of the craniomaxillofacial skeleton that included anterior maxillomandibular syngnathia and fusion of a rudimentary tongue with the soft palate.
Conclusion: This case report documents the intra-utero and pre-natal workup, perioperative management, surgical intervention, and postoperative follow-up course for an infant with documented maxillomandibular fusion.
Keywords: Craniofacial, Pediatrics, Synechiae, Syngnathia
INTRODUCTION
Congenital maxillomandibular fusion is a rare disorder of the craniomaxillofacial skeleton and soft tissue. The disorder can present as fusion of the soft tissue, also known as synechiae, or as bony fusion, also known as syngnathia. True maxillomandibular fusion without the involvement of other structures is an uncommon condition with very few occurrences documented. Syngnathia can occur in the midline, or laterally, and it can be unilateral or bilateral. Most documented cases involve a unilateral fibrous fusion [1]. The associated syndromes include oromandibular limb hypogenesis syndrome, popliteal pterygium syndrome, aglossia-adactylia syndrome, Van der Woude syndrome, cleft palate lateral alveolar synechiae syndrome [2],[3], Nager syndrome, Horner syndrome, and Dobrow syndrome. Rai et al. performed an extensive search of the literature from the year 1936 to 2018 which included a total of 118 cases with 62 cases of bony fusion, 48 cases of fibrous fusion, and 8 cases of combined fusion, i.e., fibrous at one site and bony at a secondary site [4]. Maintenance of the airway and difficulty feeding are the main concerns for such patients, which require immediate intervention because they can be fatal. We present the case of a newborn infant with intra-utero documented absence of the second through fourth digits on the right hand and micrognathia visualized on a 15-week ultrasound and verified on a 30-week ultrasound. No specific syngnathia or cleft lip or palate was noted. At birth he had congenital malformations of the craniomaxillofacial skeleton that included anterior maxillomandibular syngnathia and fusion of a rudimentary tongue with the soft palate.
CASE REPORT
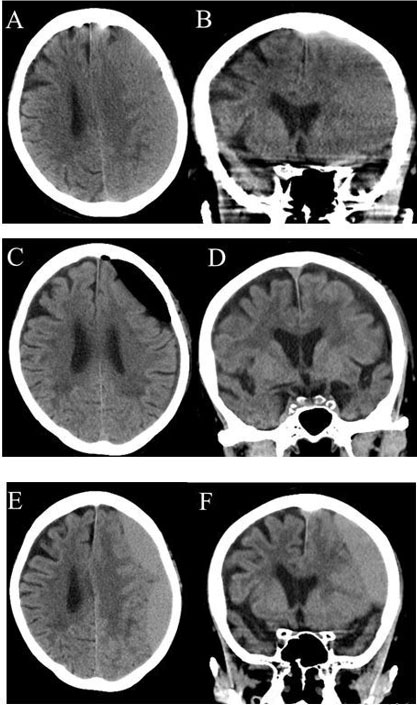
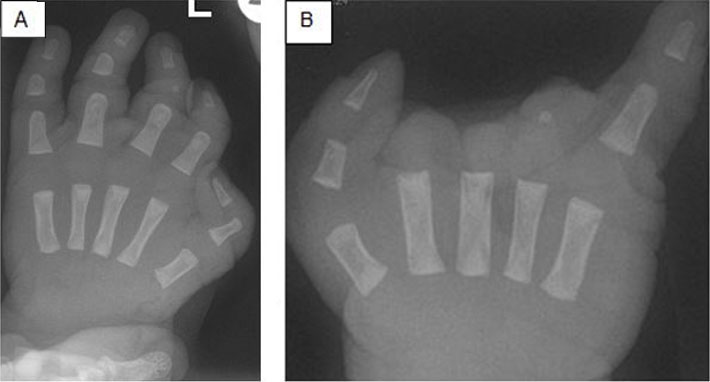
A male infant was born at 42 weeks and 2 days of gestation via cesarean section. He was the first child of an Ethiopian married couple. The mother did have appropriate prenatal care. On the initial 15-week ultrasound the developing fetus demonstrated absence of the second through fourth digits on the right hand and micrognathia. A MaterniT21 PLUS Core (LabCorp) panel was performed that was negative for Trisomy 13, 18, 21. Alpha fetoprotein screen was negative. A 30-week ultrasound again verified the hand abnormalities and micrognathia without other cranial abnormalities. A fetal echocardiogram demonstrated normal cardiac vasculature. The mother was Group B streptococcus positive and did receive appropriate treatment with Ampicillin. Otherwise, her prenatal labs were negative and there was no known teratogenic, alcohol, or tobacco exposures. At birth, the infant was noted to have micrognathia, an inability to open the mouth, and the medical team failed to pass an oral gastric tube through the mouth. The cleft and craniofacial surgery service was consulted for further management. Craniomaxillofacial anomalies included synechiae and syngnathia at the anterior mandible and premaxilla (Figure 1), micrognathia, and microstomia. Extracranial abnormalities included absence of the second through fourth digits on the right hand and left hand brachydactyly (Figure 2). Computed tomography (CT) scans of the head and neck showed no definite intracranial findings or abnormalities. An echocardiogram revealed a patent foramen ovale with a small left to right shunt and normal biventricular function.
A complete whole genome sequence and deletion/duplication analysis was performed. Genes BMPER, NRCAM, and SPEN were noted to have DNA and protein changes. Neuronal cell adhesion molecule (NRCAM) mutations are associated with neurodevelopment, neuromuscular, and skeletal abnormalities. However, genes BMPER, NRCAM, and SPEN have not been documented to have pivotal roles in maxillomandibulo-facial development [5].
In the neonatal intensive care unit (NICU), the patient was tolerating secretions and saturating well on room air. Three days after birth the patient underwent flexible nasolaryngoscopy that revealed:
- Oral Cavity Findings: Anterior maxillomandibular fusion but able to pass the bronchoscope posteriorly to visualize the airway in the region of the retromolar trigone bilaterally.
- Nasal Cavity Findings: Nasal cavities widely patent bilaterally. No obvious cleft palate on fiberoptic examination.
A nasal gastric tube was placed for feeds and the patient tolerated breast milk feeds via the nasal gastric tube. Four weeks after birth it was decided to surgically intervene on the syngnathia. The patient was brought to the operating room and a fiberoptic nasal endotracheal intubation was successfully performed by a pediatric ear nose and throat specialist. A gastric tube was placed by the general surgery team for long-term nutrition needs. Attention was then turned to the syngnathia. The gingival soft tissues were divided to reveal the anterior bone union (Figure 3).
An anterior osteotomy was then performed to divide the bone union. Once divided, a brisement procedure was performed to separate the mandible from the maxilla and gain approximately 18 mm of incisal opening (Figure 4). When the brisement procedure was performed, the rudimentary tongue was noted to be fused to the soft palate. This was then separated. The tongue was noted to be hypoplastic and underdeveloped.
The patient remained intubated to allow for a magnetic resonance image (MRI) of the head and neck to be obtained to evaluate the rudimentary tongue. The MRI revealed a genioglossus base with a small tongue (Figure 5). This is concerning for future speech and dietary needs. Of note there was no intracranial pathology noted on the MRI.
After the MRI was completed, the patient was extubated and monitored in the NICU for 72 hours with pulse oximetry and capnography to evaluate breathing pattern, breathing effort, and swallowing reflexes. The patient was able to tolerate room air and handle oral secretions. Nutrition was tolerated and supported via the gastric tube. The patient was subsequently sent to the step down floor and discharged with appropriate follow-up.
In Figure 6, he is nine months status post-surgery with self-mobilization of his lower jaw.





DISCUSSION
Syngnathia is an extremely rare condition involving abnormal development of the branchial arches. The disorder can present as fusion of the soft tissue, also known as synechiae, or as bony fusion, also known as syngnathia. Our patient presented with synostosis of the upper and lower jaw, with other head and neck pathology. This presentation can be classified as Type 1b according to Laster et al. [6]. Bony syngnathia can be found in isolation or in combination with other craniofacial (cleft lip/palate, anomalies of the tongue), vertebral, and limb malformations [7]. The pathogenesis of syngnathia is unknown. Persistence of the buccopharyngeal membrane is the most commonly cited hypothesis [8]. Other suggested mechanisms are loss or failure of migration of neural crest cells resulting in an incomplete separation of the first branchial arch into the maxilla and the mandible, lack of tongue protrusion during development, and trauma [6],[7].
CONCLUSION
Syngnathia is an extremely rare condition of unknown etiology. We report a case of anterior mandibular/maxillary syngnathia and associated limb malformations. The patient has been followed postoperatively in the craniofacial clinic. He is undergoing oral motor therapy and is being followed by infant feeding as well as speech therapy.
REFERENCE
1.
Subramanian B, Agrawal K, Panda K. Congenital fusion of the jaws: A management protocol. Int J Oral Maxillofac Surg 2010;39(9):925–9. [CrossRef]
[Pubmed]

2.
Hegab A, ElMadawy A, Shawkat WM. Congenital maxillomandibular fusion: A report of three cases. Int J Oral Maxillofac Surg 2012;41(10):1248–52. [CrossRef]
[Pubmed]
3.
Mohan A. Syngnathia-congenital maxillomandibular fusion: Case report and literature review. J Oral Maxillofac Surg 2018;76(5):1096.e1–e6. [CrossRef]
[Pubmed]
4.
Kumar V, Rattan V, Rai S. Congenital maxillomandibular syngnathia: Review of literature and proposed new classification system. J Maxillofac Oral Surg 2021;20(1):19–36. [CrossRef]
[Pubmed]
5.
Gekas J, Li B, Kamnasaran D. Current perspectives on the etiology of agnathia-otocephaly. Eur J Med Genet 2010;53(6):358–66. [CrossRef]
[Pubmed]
6.
Laster Z, Temkin D, Zarfin Y, Kushnir A. Complete bony fusion of the mandible to the zygomatic complex and maxillary tuberosity: Case report and review. Int J Oral Maxillofac Surg 2001;30(1):75–9. [CrossRef]
[Pubmed]
7.
Knoll B, Karas D, Persing JA, Shin J. Complete congenital bony syngnathia in a case of oromandibular limb hypogenesis syndrome. J Craniofac Surg 2000;11(4):398–404. [CrossRef]
[Pubmed]
8.
Gartlan MG, Davies J, Smith RJ. Congenital oral synechiae. Ann Otol Rhinol Laryngol 1993;102(3 Pt 1):186–97. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Matthew Dailey - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rick Kapitan - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Matthew Dailey et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.